Accessory Atrioventricular Pathways
By definition, accessory atrioventricular pathways are aberrant muscle bundles that connect the atrium to a ventricle outside of the regular atrioventricular conduction system. Epicardial mapping and ablation of accessory pathways through a subxiphoid approach can be an alternative when endocardial or epicardial transvenous mapping has failed.
Surgical or catheter ablation of accessory pathways by means of high-energy shocks serves as definitive therapy for patients with Wolff-Parkinson-White syndrome but has substantial associated morbidity and mortality. Radiofrequency current, an alternative energy source for ablation, produces smaller lesions without adverse effects remote from the site where current is delivered. We conducted this study to develop catheter techniques for delivering radiofrequency current to reduce morbidity and mortality associated with accessory-pathway ablation.
Clinically, they may manifest as substrates for ventricular preexcitation. The first accessory pathway in a patient who suffered from Wolff-Parkinson-White syndrome was described in 1943 by Wood, Wolferth, and Geckler.1 Shortly after, created a reconstruction of an accessory pathway that very elegantly showed the close proximity of the pathway to the fibrous attachment of the mitral valve and its relationship with the sulcus coronarius.
In the embryonic human heart, a ring of musculature at the atrioventricular canal provides myocardial continuity between developing atrial and ventricular myocardium in the early stages. This canal myocardium was shown initially to have slow conduction properties in the chick.10 The canal myocardium is sandwiched by sulcus tissue on the outside and endocardial cushions on the inside. Kim and colleagues11 showed that the bulk of the canal myocardium was incorporated into the vestibules making up the atrial walls leading toward the valvar orifices, but it did not contribute to ventricular myocardium. A small part of the canal myocardium becomes the atrioventricular node, and normally this is the only site of myocardial continuity, with the developing ventricular conduction bundles at completion of cardiac septation. In their earlier study, however, Wessels and colleagues12 noted strands of myocardial continuity between atrial and ventricular tissues in all human fetal hearts and many normal neonatal hearts.
What is known
Epicardial accessory pathways can often be ablated from a coronary venous approach but requires proximity of the vein to the pathway.
Use of a percutaneous subxiphoid approach to the pericardial space for ablation has been shown to be feasible in largely anecdotal reports.
Methods and Results
We reviewed acute and long-term follow-up of 21 patients (14 males) referred for percutaneous epicardial accessory pathway ablation. There was a median of 2 previous failed procedures. All patients were highly symptomatic, 8 had atrial fibrillation (3 with cardiac arrest) and 13 had frequent symptomatic episodes of atrioventricular reentrant tachycardia.
- Mean HR, AV conduction times
- Ventricular activation sequence
“base-to-apex”
(base ≥ 1 ms earlier than apex)
“apex-to-base”
(base ≥ 1 ms earlier than apex)
“concurrent”
(base and apex <1ms)
Immunohistochemistry: α-MLC-2a α-Periostin, α-Cx43, α-
Nkx2.5
- Location and size of APs at the developing Annulus Fibrosis
Radiofrequency current (mean power, 30.9 +/- 5.3 W) was applied through a catheter electrode positioned against the mitral or tricuspid annulus or a branch of the coronary sinus; when possible, delivery was guided by catheter recordings of accessory-pathway activation. Ablation was attempted in 166 patients with 177 accessory pathways (106 pathways in the left free wall, 13 in the anteroseptal region, 43 in the posteroseptal region, and 15 in the right free wall).
Six patients (28.5%) had a successful epicardial ablation. Five patients (23.8%) underwent a successful repeated endocardial mapping, and ablation after epicardial mapping yielded no early activation site. Epicardial mapping was helpful in guiding endocardial ablation in 2 patients (9.5%), showing that the earliest activation was simultaneous at the epicardium and endocardium.
Accessory-pathway conduction was eliminated in 164 of 166 patients (99 percent) by a median of three applications of radiofrequency current. During a mean follow-up (+/- SD) of 8.0 +/- 5.4 months, preexcitation or atrioventricular reentrant tachycardia returned in 15 patients (9 percent). All underwent a second, successful ablation. Electrophysiologic study 3.1 +/- 1.9 months after ablation in 75 patients verified the absence of accessory-pathway conduction in all. Complications of radiofrequency-current application occurred in three patients (1.8 percent): atrioventricular block (one patient), pericarditis (one), and cardiac tamponade (one) after radiofrequency current was applied in a small branch of the coronary sinus.
Four patients (19%) underwent successful open-chest surgery after failing epicardial/endocardial ablation. Two patients (9.5%) remained controlled under antiarrhythmic drugs after unsuccessful endocardial/epicardial ablation. Two patients had a coronary sinus diverticulum and one a right atrium to right ventricle diverticulum. Three patients acquired postablation coronary sinus stenosis. There was no major complication related to pericardial access.
Anteroseptal Accessory Atrioventricular Pathways
Accessory pathways were classified as anteroseptal in location if the accessory-pathway activation potential and the His-bundle potential were recorded by the same close bipolar electrode.
Ablation of an Anteroseptal Accessory Atrioventricular Pathway.). To minimize the risk of atrioventricular block, radiofrequency current was delivered on the ventricular side of the tricuspid annulus. The ablation catheter was inserted through the right subclavian venous sheath and curved beneath the septal or anterior tricuspid leaflet. If this approach was unsuccessful, an ablation catheter was inserted through the right femoral venous sheath and placed parallel to the His-bundle catheter.
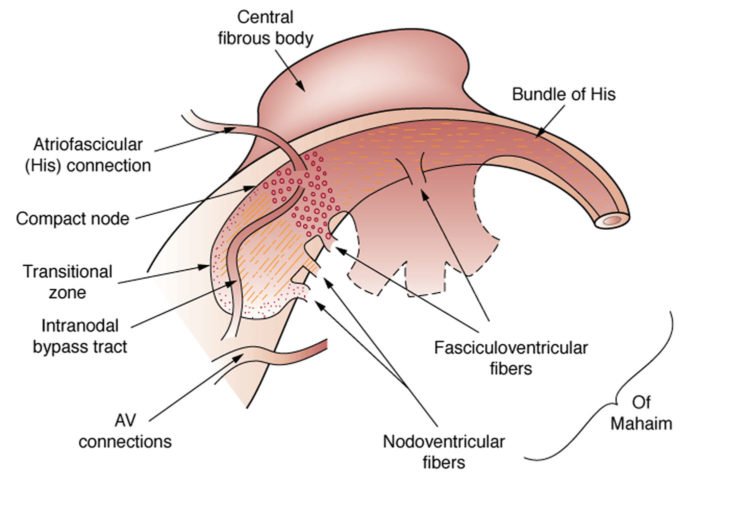
Conduction from the atria to the ventricles normally occurs via the atrioventricular node (AV)-His-Purkinje system. Patients with a preexcitation syndrome have an additional or alternative pathway, known as an accessory pathway, which directly connects the atria and ventricle and bypasses the AV node. AV conduction through an accessory pathway (most commonly a direct AV connection) results in the earlier activation of the ventricles than if the impulse had traveled through the AV node; hence the term preexcitation.
Accessory pathway is a generic term which may indicate either a “tract” which bypasses the AV node but inserts into the specialized conduction system (eg, the bundle of His, right or left bundles, or one of the fascicles), or a “connection” which bypasses the AV node and terminates directly within the myocardium. Other names that may be used include anomalous AV pathway, connection, or tract; accessory AV bypass pathway, connection, or tract; or simply AV bypass, tract, or pathway.
Design—The conduction properties of the AP and the AV node were studied in 356 patients with single manifest AP who underwent successful ablation.
Objective—The objective of this study was to determine the conduction properties of the nOlmal atrioventricular (AV) conduction system in relation to accessory pathway (AP) location in patients with symptomatic Wolff–Parkinson–White syndrome.
Multiple Accessory Atrioventricular Pathways
Two separate accessory pathways were considered to be present if sites where radiofrequency current affected accessory-pathway conduction were separated by more than 3 cm.
Post-Ablation Managementk
Thirty to 60 minutes after the final application of radiofrequency current, complete atrial and ventricular stimulation was repeated to verify the absence of accessory-pathway conduction and to exclude the presence of another accessory pathway and other arrhythmias, such as atrioventricular nodal reentrant tachycardia. Heparin administration was resumed 3 hours after the procedure and maintained for 48 hours in the first 27 patients with left—free-wall accessory pathways. Heparin was not administered after the procedure in the remaining patients. Transesophageal echocardiography was performed 18 to 72 hours after the ablation procedure to exclude thrombi at the ablation sites. Patients were discharged on the second day after ablation except for the 27 patients who received heparin, who were discharged on the third day after ablation. Patients were followed by the investigators or by the referring physician, and it was recommended that a follow-up electrophysiologic study be performed two to three months after ablation.
Posteroseptal Accessory Atrioventricular Pathways
For posteroseptal accessory pathways, the ablation catheter was positioned in one of the following ways: (1) through the right femoral venous sheath, with the tip electrode placed against the tricuspid annulus or around the margin of the coronary-sinus ostium; (2) through the right femoral artery, with the tip electrode positioned against the mitral annulus, close to the septum, as in the approach used for left—free-wall pathways; or (3) through the right subclavian venous sheath, with the tip electrode positioned in a venous branch of the proximal coronary sinus (i.e., the middle cardiac vein).
For more information visit us our website: https://www.healthinfi.com
0 200
No Comments