
About Primary Biliary Cirrhosis (PBC)
Primary biliary cirrhosis (PBC) is a progressive disease of the liver caused by a buildup of bile within the liver (cholestasis) that results in damage to the small bile ducts that drain bile from the liver. Over time, this pressure build-up destroys the bile ducts leading to liver cell damage.
As the disease progresses and enough liver cells die, cirrhosis and liver failure occur.
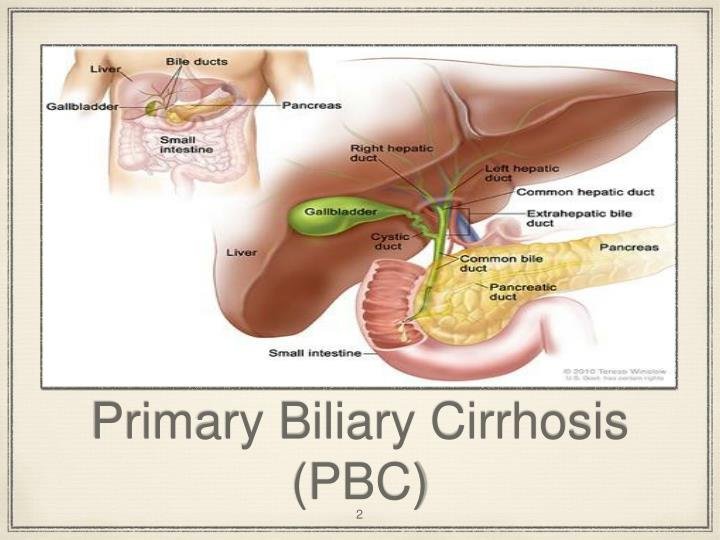
Bile is manufactured in the liver and then transported through the bile ducts to the gallbladder and intestine where it helps digest fats and fat soluble vitamins (A,D,E,K).
When bile cannot be drained from the liver, it causes inflammation that leads to cell death. Scar tissue gradually replaces the areas of damaged liver and then the body cannot perform necessary functions.
Primary biliary cirrhosis (PBC) is a presumed autoimmune disease of the liver, which predominantly affects women once over the age of 20 years. Most cases are diagnosed when asymptomatic (60%). The antimitochondrial antibody is present in serum in most, but not in all, patients with PBC.
The disease generally progresses slowly but survival is less than an age- and gender-matched general population.
The symptomatic patient may have fatigue, generalized pruritus, portal hypertension, osteoporosis, ,skin xanthomata, fat soluble vitamin deficiencies, and/or recurrent asymptomatic urinary tract infections. Many nonhepatic autoimmune diseases are found in association with PBC and may prompt initial presentation.
To date, immunosuppressive therapy has not been shown to prolong survival in PBC. The hydrophilic bile acid, ursodeoxycholic acid (UDCA), has been shown when given in a dose of 13 to 15 mg/kg daily for up to 4 years to delay the time to liver transplantation or death.
This therapy also causes a significant improvement of all the biochemical markers of cholestasis but has no beneficial effects on any of the symptoms or associated disorders. Treatment with UDCA does not obviate the need for liver transplantation.
Therapies to prevent complications arising from malabsorption, portal hypertension, and/or osteoporosis are required as well. Good control of pruritus can be achieved in most patients.
PBC is diagnosed with increasing frequency, but the agent(s) responsible for this slowly progressive destruction of the interlobular bile ducts remains elusive and hence a specific therapy remains unavailable. (HEPATOLOGY 2000;31:1005-1013.)
are designed to aid the practicing physician in diagnosing PBC, establishing the severity of the disease, recognizing the direct complications of PBC and its associated disorders, and finally, to advise on the therapies available that will benefit patients from a symptomatic, preventative, and therapeutic standpoint.
As such, what is written should be taken as guidelines and not ‘‘standards of care.’’ The strength of each recommendation is categorized based on the quality of evidence in the literature according to the rating system indicated in Table 1.
Where appropriate throughout this report, categories A through E have been attached to the recommendations to indicate the benefit to be expected from following the suggested recommendations.
PBC is a presumed autoimmune disease of the liver, which predominantly affects middle-aged women.2 PBC is caused by granulomatous destruction of the interlobular bile ducts, which leads to progressive ductopenia. The consequent cholestasis is generally slowly progressive, and fibrosis, cirrhosis, and eventual liver failure occur.
Currently, the diagnosis of PBC most often is made when the patient is still asymptomatic, with abnormal liver biochemistry and/or antimitochondrial antibodies (AMA) noted in blood at the time of a routine check-up or as part of the work-up for an associated disorder.
Elevation in serum alkaline phosphatase (ALP) (with confirmation of hepatic origin by checking the gamma glutamyl transpeptidase [gGT]) is the most common biochemical abnormality in PBC. Although at diagnosis few patients have elevation of their serum bilirubin; when present, it should be the conjugated fraction that is elevated.
Elevation of serum bilirubin is a late phenomenon and an excellent predictor of survival.3 As in any patient with chronic cholestasis, total serum cholesterol may be elevated.
Signs and Symptoms
Some of the more common symptoms and signs of cirrhosis include:
- Yellowing of the skin (jaundice) due to the accumulation of bilirubin in the blood
- Fatigue
- Weakness
- Loss of appetite
- Itching
- Easy bruising from decreased production of blood clotting factors by the diseased liver.
Treatment
The only “cure” for primary biliary cirrhosis is liver transplant, but it is only considered as a treatment option if other less aggressive treatments have failed and the patient develops liver failure.
Ursodiol (Actigal) or ursodeoxycholic acid (UDCA) is the first line treatment for PBC. It helps the liver transport bile into the gallbladder and intestine, in an attempt to prevent cholestasis.
Depending upon the severity of the disease, immune suppression medications may be prescribed, including methotrexate (Rheumatrex, Trexall), cyclosporine and prednisone.
Itching may be intense and difficult to control. Antihistamines like diphenhydramine (Benadryl) may be helpful but other drugs may be considered including cholestyramine (Questran, Questran Light), which helps bind bile and decrease the itching associated with elevated bilirubin levels in the blood.
Complications of PBC will need to be cared for. These include cirrhosis, portal hypertension, gastrointestinal bleeding, osteoporosis, and vitamin deficiencies.
What is the prognosis for someone with primary biliary cirrhosis?
PBC is a progressive disease that can be controlled but not cured. The prognosis depends upon a variety of factors including whether the patient has symptoms (especially fatigue), liver function test abnormalities, and whether the patient has undergone treatment with medication or has required liver transplantation.
Advances in treatment have extended the life expectancy in the past many years. The average survival from diagnosis for a patient with PBC who is asymptomatic is 16 years, while that of patients with symptoms is 7 1/2 years.
Can primary biliary cirrhosis be prevented?
Since the cause of the disease is not known, it is not possible to prevent PBC. However, medications may be able to slow the progression of the disease and control the symptoms.
Should a person develop PBC, all attempts should be made to prevent further potential damage. This may include limiting alcohol intake, avoiding the use of medications that contain acetaminophen (Tylenol, Panadol), and cholesterol lowering agents.
What are the risk factors for primary biliary cirrhosis?
- There may be a genetic component to the development of PBC since a person with the disease is likely to have a family member also afflicted.
- Women are nine times more likely than men to develop PBC. It most often develops in the middle age between the ages of 40 to 60.
- The disease is seen more often in white, northern Europeans, compared to African-Americans.
Manifestations Of PBC Associated Disorders
The prevalence of autoimmune disorders found in association with PBC is reported in several large series.
- Thyroid dysfunction is a common autoimmune disorder associated with PBC and its presentation often predates the diagnosis of PBC.
- If sicca symptoms are sought by direct questioning, they are present in up to 70% of PBC patients.53 Symptoms related to the sicca syndrome include xerophthalmia, xerostomia, dental caries, dysphagia, tracheobronchitis, and dyspareunia.
If a superimposed motility problem is also present, asymptomatic or symptomatic reflux causing esophagitis and possible stricture formation may develop. This is more common in patients with the CREST syndrome.
- CREST (calcinosis cutis, Raynaud’s phenomena, esophageal dysmotility, and telangiectasia) in its complete form is rarely seen in PBC patients.
- Raynaud’s syndrome alone is more common and is particularly troublesome for patients living in cold climates.
- Rheumatoid factor is present in the serum in 25% of patients with PBC, but symptomatic arthritis is less common.
- Celiac disease, often asymptomatic, is present in 6% of PBC patients.
- Inflammatory bowel disease, namely ulcerative colitis may be uncommonly seen in association with PBC.


No Comments