Chronic Myelomonocytic Leukemia (CMML
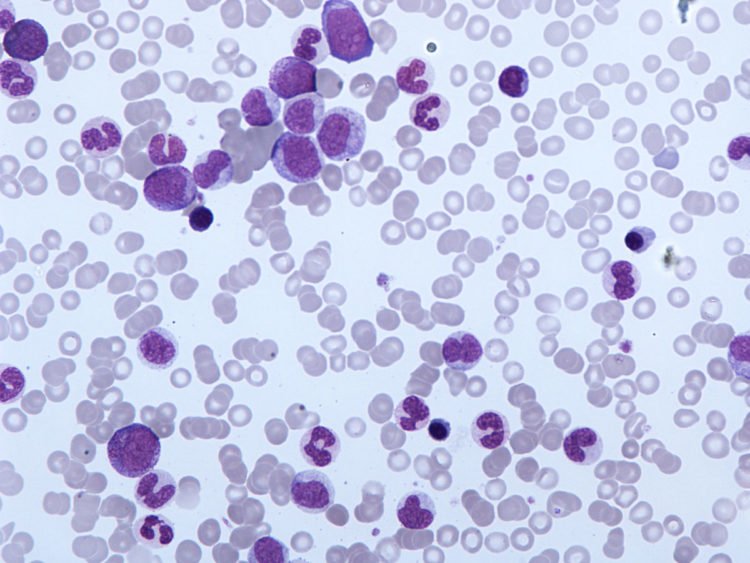
CMML is a type of leukemia that is portrayed by high quantities of white platelets, called ‘monocytes’, in the blood and bone marrow.
CMML is an exceptional blood disease with highlights of two different kinds of blood malignancy. Despite the fact that it has leukemia as a major aspect of its name, the World Wellbeing Association (WHO) arranges CMML as a ‘blended myelodysplastic (MDS) myeloproliferative neoplasm (MPN). MPN is a gathering of clutters of the bone marrow immature microorganisms that create abundance quantities of at least one sorts of platelets (red cells, white cells, or platelets). MDS is a gathering of illnesses that effects, to a more prominent or lesser degree, the creation of typical platelets in the bone marrow.
Around half of individuals analyzed have a kind of CMML with a high white cell tally and look like a MPN. The other half have an ordinary or decreased white cell tally at analysis and the illness is more like a MDS. CMML is distinctive to endless myeloid leukemia (CML).
CML influences the myeloid cells in the blood and bone marrow, while CMML influences a particular myeloid cell called a monocyte, which battles contaminations.
Unending myelomonocytic leukemia (CMML) begins in the bone marrow and after that moves to the blood. It happens when monocytes in the bone marrow start to become wild, filling the bone marrow and keeping other platelets from developing.
CMML is uncommon, happening in around 4 of each 1 million individuals in the U.S. every year, with around 1,100 new cases analyzed every year. Around 9 out of 10 cases are found in individuals 60 and more established. CMML happens more frequently in men than in ladies and is exceptionally uncommon in youngsters.
CMML used to be viewed as a kind of myelodysplastic disorder (MDS) since patients have anomalous looking (dysplastic) cells in their bone marrow. Yet, different elements related with CMML didn’t coordinate the meaning of MDS. Rather, they all the more nearly took after myeloproliferative neoplasms, a gathering of ailments where the bone marrow makes an excessive number of cells. Since CMML has highlights of both myelodysplastic disorder and myeloproliferative neoplasm, specialists made another “cover” classification of myelodysplastic/myeloproliferative neoplasm.
In the vicinity of 15 and 30 percent of CMML patients go ahead to create intense myeloid leukemia (AML).
Signs and Symptoms
The most common sign of chronic myelomonocytic leukemia (CMML) is having too many monocytes (seen on a blood test).
Having too many monocytes also causes many of the symptoms of CMML. These monocytes can settle in the spleen or liver, enlarging these organs. An enlarged spleen (called splenomegaly) can cause pain in the upper left part of the belly (abdomen). It can also cause people to notice they feel full too fast when they eat. If the liver gets too big (called hepatomegaly), it causes discomfort in the upper right part of the abdomen.
Low numbers of other types of blood cells cause many of the signs and symptoms of CMML: A shortage of red blood cells (anemia) can lead to feeling very tired, with shortness of breath and pale skin.
Not having enough normal white blood cells (leukopenia) can lead to frequent or severe infections. A shortage of blood platelets (thrombocytopenia) can lead to easy bruising and bleeding. Some people notice frequent or severe nosebleeds or bleeding from their gums.
Other symptoms can include weight loss, fever, and loss of appetite. Of course, many of these problems are caused more often by something other than cancer. If you’re having symptoms, you should see a doctor so a cause can be found.
Causes of CMML
The exact cause of CMML is not known. There are, however, known risk factors that increase the chances of getting CMML. They include:
- Older age (60 or older)
- Being male
- Being exposed to certain chemicals at work or in the environment
- Being exposed to radiation
- Past treatment with certain anticancer drugs
We do not know the cause of CMML. We do know that some cases of CMML occur as a result of a gene mutation. Gene mutations known as TET 2 and RAS have been linked to CMML. Potentially, any incident that damages the genetic material of the body can cause a mutation that may lead to the development of CMML.
Examples of these incidents may include:
- ageing
- cytotoxic chemotherapy
CMML is not infectious and cannot be transmitted from one person to another.
Diagnosing CMML
Many people are diagnosed after having a blood test for another problem.When abnormal monocytes are found, further tests are organised:
- further blood tests
- bone marrow biopsy
- cytogenetic tests.
What is the Prognosis for the Disorder?
Overall, CMML patients have a median overall survival of 20-40 months with highly heterogeneous subgroups contained within the overarching diagnosis. Multiple scoring systems have been developed to better predict which patients will do better or worse. In most systems, even the best prognosis group has a mean overall survival between 2 and 3 years.
In the M.D. Anderson prognostic scoring system for CMML, the best prognosis subgroup showed a median overall survival of 24 months, whereas the worst was at 5 months, with intermediate groups falling at 15 and 8 months. Poor prognostic factors in this analysis were hemoglobin less than 12 g/dL, lymphocytosis greater than 2,500/ microliter, circulating immature myeloid cells, and blasts greater than or equal to 10% of bone marrow.
The Dusseldorf scoring system is based on hemoglobin less than 9g/dL, platelets less than 100,000/ microliter, increased lactate dehydrogenase (LDH), and bone marrow blasts greater than 5%.
Of note, although the best prognostic group had a median survival of more than 90 months, only 6% of patients were classified into this group. The other subgroups, representing 94% of patients, showed 26- and 11-month median overall survival times. In the other major scoring systems, increased blasts, decreased hematopoietic function, and increased LDH are all poor prognostic factors and yield similar groupings of patients.
Death in CMML is due to AML transformation in 20% of cases. Infection (30%), bleeding (20%), heart failure (10%), other CMML-related causes (10%), and non-CMML-related causes (10%) represent the remainder.
The only curative therapy for CMML is allogeneic bone marrow transplantation, although newer pharmaceutical approaches with RAS inhibitors and histone deacetylation inhibitors are being pursued.
CMML treated
Treatment of CMML depends on how severe the disease is, as well as the patient’s age and health. Treatment options include:
- Supportive carewith blood transfusions, growth factors and antibiotics to treat symptoms by increasing blood counts and stopping infections
- Chemotherapyto kill cells cancer cells using cytotoxic agents
- Radiation therapy with high-energy rays or particles to destroy cancer cells
- Stem cell transplant, which replaces blood-forming stem cellsin your bone marrow with healthy stem cells from a donor
Clinical trials, also called research studies may offer good treatment options for some people with CMML. These studies also help researchers better understand the value of promising new treatments or procedures.
There is no one standard treatment regimen for CMML. Treatment depends on factors including: the stage of the disease; a person’s age; the extent of symptoms; and general overall health. People with MDS-type CMML and MPN-type CMML usually are treated with the same or similar chemotherapy drugs to control the disease. CMML is often managed using the ‘watch and wait’ approach, with supportive care provided if and when required.
Watch and Wait” involves regular monitoring of blood and general health. No intervention is needed unless the person begins developing signs and symptoms of the disease, indicating it is progressing.
Supportive care refers to the administration of therapies to alleviate symptoms of the disease or to manage the side-effects of the therapies. Supportive care is aimed at improving the person’s quality of life and may even extend the person’s life. This is often the only treatment suitable for older people, or those with other health problems, as they may be less able totolerate stronger treatments. The aim of supportive care is not to treat the disease but to alleviate symptoms such as shortness of breath, bruising or bleeding.
Supportive care therapies may include:
- Blood and platelet transfusions -Transfusing blood products may be required to alleviate symptoms and to improve overall health.
- Antibiotics – People who have a reduced immune system from CMML may be at an increased risk of developing severe infection. Antibiotics can prevent a simple infection becoming life threatening.
- Chemotherapy involves the use of chemicals. Chemotherapy drugs are also known as cytotoxic(cell toxic) as they kill cells, especially those that multiply quickly, like cancer cells. Chemotherapy can be given as a tablet, as an infusion into the vein, or as an injection under the skin. Recently, azacitidine has been used to treat CMML.


No Comments