
Overview
A stroke—also referred to as a brain attack—occurs when a part of the brain is injured by a disturbance to its blood supply.
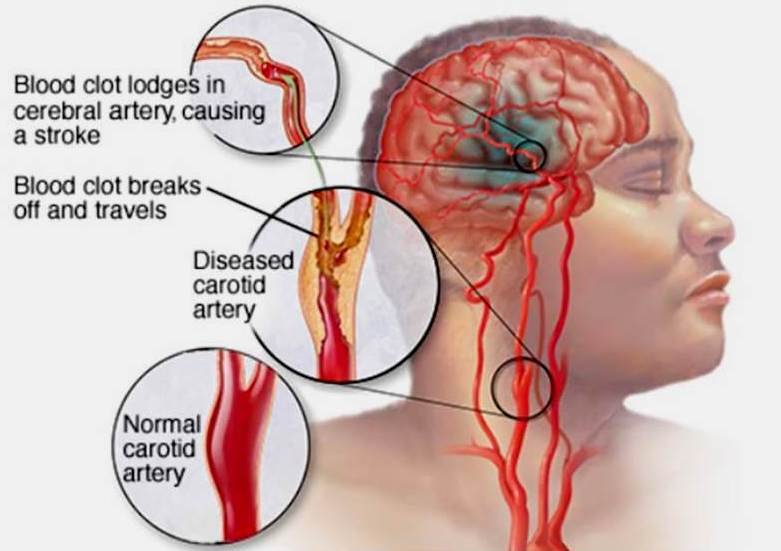
There are two types of stroke. An ischemic stroke, or cerebral infarction, occurs when the flow of blood through an artery supplying part of the brain is suddenly interrupted, usually by a clot. A hemorrhagic stroke, or intracerebral orsubarachnoid hemorrhage, occurs when a blood vessel in the brain bursts, releasing blood into the substance of the brain or into the spaces surrounding the brain.
The term “brain attack” is becoming increasingly common to describe this condition. A person suffering a loss of blood flow to the heart is said to be having a heart attack, so a person with a loss of blood flow to the brain or sudden bleeding in the brain is having a “brain attack.” Deprived of oxygen, nerve cells (neurons) in the affected area of the brain can’t function and die within minutes. And when nerve cells can’t function, the part of the body controlled by these cells can’t function either. Although the healing process can help some patients improve after a stroke, some devastating effects of stroke are often permanent; unlike other cells in the body, dead brain cells aren’t replaced.
Strokes affect different people in different ways, depending on the type of stroke, the area of the brain affected and the extent of the brain injury. Brain injury from a stroke can affect speech and language, motor activity (muscles and strength), cognitive ability, behavior, memory and emotions. Paralysis or weakness on one side of the body is common. Stroke is the leading cause of serious adult disability.
More women than men suffer strokes. In 2006, women accounted for about 60 percent of stroke deaths. And of the 6.4 million stroke victims who are alive today, 2.5 million are males and 3.9 million are females. Of every 10 deaths from stroke, six occur in women and four in men. This is because the average life expectancy for women is greater than for men, and the highest rates for stroke are in the oldest age groups.
Stroke is often deadly: the condition killed more than 137,000 Americans in 2006, accounting for one in 17 deaths. Stroke ranks third after heart disease and cancer as a major cause of death in the United States.
The most important risk factors for stroke are hypertension, heart disease, diabetesand cigarette smoking. Other factors that increase your risk of having a stroke include heavy alcohol consumption, high cholesterol levels, migraines (especially with aura), illicit drug use and genetic or congenital conditions (particularly vascular abnormalities).
Atrial fibrillation, a heart rhythm disturbance that causes the small chambers of the heart to beat irregularly allowing blood clots to form, is another risk factor. It is particularly common in elderly people; it increases markedly in people after age 65, and it affects about 9.8 percent of women and 12.2 percent of men 65 and older. It may also occur in younger women, particularly in association with hyperthyroidism or Graves’ disease. However, you can have a stroke at any age. More than a quarter of stroke victims are under 65.
Stroke risks may be common in some families, particularly those in which family members have had heart attacks before age 50. These families have a tendency for premature atherosclerosis, or “hardening of the arteries,” and may share a genetic predisposition for high blood pressure, elevated cholesterol or diabetes, all of which are risk factors for stroke. Of course, shared lifestyle habits of poor diet, lack of exercise and tendency to smoke or drink may also be a factor in a family history of stroke.
African Americans are more likely to have strokes than Caucasians, but after age 55 the risk of death from stroke is the same for Caucasians as for African Americans. Researchers note that African Americans have higher rates of stroke risk factors, including high blood pressure, cigarette smoking, diabetes and sickle cell anemia. It is not clear whether the increased risk of stroke in minority populations is related to increased prevalence of these risk factors or to other factors. Hispanic Americans and Native Americans also have an increased risk of stroke, which may also relate to their higher rates of stroke risk factors, including diabetes and hypertension.
Some risk factors for stroke apply only to women, including pregnancy, childbirth (especially the postpartum period) and menopause. These risk factors are tied to hormonal fluctuations, changes in blood volume, tendency to form blood clots and other physical changes that affect a woman in different stages of life.
Some studies have shown an increased risk of stroke in pregnancy, particularly in pregnant women who suffer complications such as preeclampsia and postpartum hemorrhage. The period immediately after delivery (the postpartum period) is the period of highest stroke risk. During this time, there is an increasing tendency to form blood clots, which can lead to clots in the veins of the brain. This can cause headaches, seizures, brain swelling, bleeding in the brain and loss of function.
A 2005 study published in the journal Obstetrics and Gynecology found that women with pregnancy complications were nearly 75 percent more likely to suffer a stroke in the 13.5 years following their pregnancies than women with no pregnancy complications. However, since the risk of stroke in women of childbearing age is very small to begin with, a moderate increase in risk during pregnancy is still a relatively small risk.

Migraine, particularly when it is associated with aura (loss or change in vision preceding the headache), is also more common in women than men, and it has been associated with an increased risk of stroke. Because the increased risk is small, however, very few women with migraine will ever suffer strokes. The combination of migraine, smoking and oral contraceptive use can act together to increase the risk further, however.
Having already had a stroke puts you at higher risk for another one. Recurrent stroke is frequent: about 25 percent of people who recover from a first stroke will have another one within five years. The risk of severe disability or death from stroke increases with each stroke recurrence, and the risk of recurrence is greatest soon after a stroke. According to the National Institutes of Health, about three percent of stroke patients will have another stroke within 30 days of their first one, and one-third of recurrent strokes take place within two years of the first stroke. The underlying cause of the stroke influences the risk of recurrence.
A transient ischemic attack (TIA), sometimes called a ministroke, also is a risk factor for stroke. A TIA starts just like a stroke, lasts several minutes and then symptoms disappear. You should still contact your doctor immediately because there is no way of telling if the episode will be a TIA or a full-blown stroke. And, even if it is a TIA, you may be able to prevent a more serious stroke.
An additional risk factor applies only to people subject to hemorrhagic stroke. A person with an abnormality of the brain blood vessels, such as an aneurysm orarteriovenous malformation (AVM), is at increased risk for hemorrhagic stroke. Aneurysms are weakened blood vessels that balloon out on the blood vessel wall, while AVMs are a tangle of defective blood vessels and capillaries in the brain. Both have areas of thin walls and are more likely to rupture.
Types of Stroke
Stroke is actually a collective term for many subtypes of brain injuries:
- Ischemic strokes are caused by blood clots. There are two types of ischemic stroke:
- Embolic stroke means a blood clot forms somewhere in the body (either in the heart or in one of the arteries in the chest or neck that supply the brain) and travels through the bloodstream to your brain.
- Thrombotic stroke means the blood flow ceases because of a blockage of one or more of the arteries supplying blood to the brain or within the brain itself.
- Hemorrhagic results when a blood vessel bursts in the brain. Two types of hemorrhagic stroke include:
- Intracerebral hemorrhage occurs when vessels bleed within the brain itself.
- Subarachnoid hemorrhage is usually caused by the rupture of an aneurysm or a malformation of blood vessels on or near the thin, delicate membrane surrounding the brain.
Clotting is a necessary function; it stops bleeding and allows repair of damaged areas of arteries or veins. However, when arteries are damaged by atherosclerosis (“hardening of the arteries”), the lining of the artery is injured and cholesterol components seep into the wall of the blood vessel.
This sets up an inflammatory response within the vessel wall and ultimately forms aplaque. Plaque rupture attracts blood-clotting factors that can interfere with blood flow to the brain. A thrombotic stroke or cerebral thrombosis is caused by thrombosis, the formation of a blood clot on top of an atherosclerotic plaque, which grows large enough to block blood flow. Atherosclerotic plaques can start to develop in young adulthood but may take several decades to produce stroke symptoms. Atherosclerosis progression is accelerated by conditions such as hypertension, diabetes, smoking and hypercholesterolemia.
A clot can also form in another part of the body, such as the heart, and travel through blood vessels and become wedged in a brain artery. This free-roaming clot is called an embolus. A stroke caused by an embolus is called an embolic stroke.
A transient ischemic attack (TIA) starts just like a stroke but goes away after several minutes with no lasting damage. Recent evidence suggests that many patients with TIA actually do have small strokes: as many as one-third of those whose symptoms last less than an hour. You can’t ignore it. Even if it is a TIA, take heed: it can be a warning that you are at risk for a more serious stroke.
According to the American Heart Association, more than one-third of Americans who have a TIA will have an acute stroke sometime in the future. However, TIAs are a better prediction of if a stroke will happen than when; a stroke may occur days, weeks or months after a TIA. In about half of cases, the stroke takes place within a year of the TIA. Thus, the occurrence of a TIA should be taken very seriously, and you should seek medical attention immediately to prevent a disabling stroke.
Hemorrhagic stroke accounts for about 13 percent of all strokes and is more frequent among the young and people with high blood pressure. One common cause is a bleeding aneurysm (weak or thin spot on an artery wall). Over time, these weak spots stretch or balloon out under high pressure. The thin walls of these ballooning aneurysms can rupture and spill blood into the space surrounding brain cells.
Hemorrhage also can occur when arterial walls break open. Plaque-encrusted artery walls eventually lose their elasticity and become brittle, thin and prone to cracking. High blood pressure increases the risk that a brittle wall will give.
When an artery in the brain bursts, blood spews into the surrounding tissue. Brain cells generally don’t come into direct contact with blood; the contact upsets the delicate chemical balance neurons require to function. For people with hemorrhagic strokes, treatment is aimed at alleviating pressure on the brain and minimizing damage.
As the terms “brain attack” and “stroke” suggest, strokes strike suddenly. Symptoms include numbness or weakness of the face, arm or leg, especially on one side of the body; confusion; difficulty speaking or understanding speech; trouble seeing out of one or both eyes; dizziness, or loss of balance or coordination; or sudden, uncharacteristic, severe headache, which is most characteristic of bleeding. Since the symptoms appear suddenly and there is usually more than one, you can often distinguish stroke from other causes of dizziness or headache.
Brain cells die when they no longer receive oxygen and nutrients from the blood, but they also are damaged by sudden bleeding into or around the brain. When blood flow to the brain is interrupted, some brain cells die immediately, while others remain at risk for dying. That’s why immediate treatment is critical.
If you experience the sudden onset of the worst headache in your life or a sudden onset of neurological symptoms, call 911 and get to a hospital immediately . Do not waste precious time by calling your health care professional and do not call a family member. These actions have been shown to cause unnecessary delays in treatment. The best action is to call 911. The most effective therapies must be administered fast—typically within three hours of when the stroke started.
Although some health care professionals suggest taking aspirin at the onset of a heart attack, this recommendation hinges on the type of stroke you suffer, and it isn’t a remedy you should take into your own hands. Don’t take aspirin in a stroke situation without advice from a health care professional.
Diagnosis
Being aware of a stroke’s warning symptoms is the first step in diagnosis and management. Symptoms vary depending on the area of the brain that is involved, but they are still relatively easy to identify.
Primary symptoms include:
- sudden, painless numbness or weakness, usually on one side of the body
- sudden confusion or trouble speaking or understanding speech
- sudden trouble seeing out of one or both eyes
- sudden trouble walking
- dizziness or loss of balance or coordination
- sudden severe headache with no known cause
Notice the one oft-repeated word: sudden. When you’re having a stroke, time is critical. Recognizing a stroke quickly means you get help sooner and may be able to minimize the amount of damage the stroke will cause.
You may experience other, less-common symptoms, including sudden nausea, fever and vomiting. Sometimes, a stroke is accompanied by fainting, convulsions or coma. Stroke symptoms do not cause pain in the limbs, but hemorrhagic strokes are typically associated with sudden, severe, uncharacteristic headache.
If you’re having a stroke, you should get to the hospital as soon as possible. Once you get there, health care professionals will obtain basic vital information such as blood pressure and heart rate and will begin a neurological examination. One standardized way of reporting the neurological problems and the severity of a stroke is the standardized National Institutes of Health (NIH) Stroke Scale, developed by the National Institute of Neurological Disorders and Stroke (NINDS). Health care professionals use the NIH Stroke Scale to measure a patient’s neurological deficits by asking the patient to answer questions and to perform several physical and mental tests.
Health care professionals also use a variety of imaging devices to evaluate stroke patients. The most widely used imaging procedure is the computed tomographic (CT) scan. It creates a series of cross-sectional images of the head and brain. Since it works quickly and is generally available 24 hours a day at most hospitals, the CT scan is usually one of the first tests given to patients suspected of having a stroke. It can rule out a hemorrhage and reveal if a tumor or other problem is causing the symptoms.
If a stroke is caused by hemorrhage, a CT can show evidence of bleeding into the brain immediately after stroke symptoms appear. This is important, since a stroke caused by a hemorrhage must be treated differently than one caused by a blood clot. For instance, the only proven acute stroke therapy for ischemic stroke is thrombolytic therapy, or the use of medications to dissolve or break up blood clots. This therapycannot be used until the doctor diagnoses you with an ischemic stroke. Otherwise, the treatment could make a hemorrhagic stroke worse by increasing bleeding.
Your doctor may also order a magnetic resonance image (MRI) , which uses magnetic fields to detect subtle changes in brain tissue content. The benefit of MRI over CT imaging is that MRI is better able to detect small areas of dead cells soon after the stroke begins.
Other tests include angiography, ultrasound and magnetic resonance angiography (MRA), all of which can detect blockage of brain arteries.
Risk Factors
Determining if you have any of the risk factors associated with stroke can help your health care professional estimate your likelihood of having one over many years.
The most important risk factors for stroke are high blood pressure, heart disease, diabetes and cigarette smoking. Others include heavy alcohol consumption, high cholesterol levels, illicit drug use and genetic conditions, particularly those involving the blood vessels. Significant trauma to the head or neck can cause a rip to form in the wall of the artery, called a dissection, increasing the risk of stroke, while bacterial and viral infections are also associated with stroke.
One potential risk factor for stroke is chiropractic manipulation. A study published in a 2003 issue of Neurology suggested that people who undergo chiropractic neck and spine adjustments may have a higher risk of stroke as a result of tiny tears in their arteries. The study found that patients under 60 who had strokes or ministrokes from tears in their neck arteries were more likely to have visited a practitioner who manipulated their neck within the past 30 days compared with people who had strokes from other causes.
The authors warned that a significant increase in neck pain following spinal manipulation warrants immediate medical evaluation. This was a retrospective study, however, in which patients were asked to remember events that occurred months or even years before. Very few people who go for chiropractic manipulation experience strokes.
Although there may not be a single genetic factor associated with stroke, genes do play a large role in hypertension, heart disease, diabetes and vascular malformations. (Of course, genes may not be the ultimate culprits. Increased risk for stroke within a family might be due to a common lifestyle issues such as lack of exercise or poor eating habits.)
Treatment
The type of treatment you receive depends on the type of stroke you suffered and how long it has been since the stroke started. The three phases of treatment for stroke are: prevention, therapy immediately after stroke, and post-stroke rehabilitation. Therapies for stroke include medications, surgery and rehabilitation.
The most popular classes of drugs used to prevent or treat stroke are antithrombotics (antiplatelet agents and anticoagulants) and thrombolytics.
Thrombolytic agents (clot-busters) are used to treat an ongoing, acute ischemic stroke caused by an artery blockage. These drugs act by dissolving the blood clot blocking blood flow to the brain, thus restoring, or reperfusing, the brain’s blood flow. The only FDA-approved thrombolytic for the treatment of stroke is recombinant tissue plasminogen activator (tPA), a genetically engineered form of a thrombolytic substance made by the body.
TPA can be effective if given intravenously within three hours of the start of the stroke but can only be given after confirming the stroke is ischemic, not hemorrhagic, typically with a CT scan. A major clinical stroke trial (ECASS- III ) recently found that tPA can be effective even when given up to 4½ hours after ischemic stroke in carefully selected patients.
More specifically, in 3,570 patients who received either tPA or a placebo, the chances of a good outcome at three-months was more than double for those who received tPA within 90 minutes of a stroke, 68 percent higher in those who received tPA between 90 minutes to three hours and 28 percent higher in those treated with tPA between three and 4½ hours. As a result, in 2009, the American Stroke Association revised its recommendations and now says tPA can be given up to 4½ hours after stroke symptoms in some patients.
Strokes caused by bleeding—hemorrhagic strokes—cannot be treated with tPA because the drug would make the bleeding worse and could be fatal.
Another treatment for people with acute ischemic stroke involves the use of a special corkscrew-type device to pull out a blood clot from the blood vessel in the brain where the blockage exists. The device is delivered by a catheter, or narrow tube, carefully threaded through the femoral artery in the groin up through the body to the brain. This type of highly specialized procedure can only be performed at certain medical centers and by those experienced in its use, and it must be performed within eight hours of the onset of the stroke. Other similar devices that can be used to flush the clot out of the brain blood vessel have also been approved recently. Doctors may choose to use a combination of these devices in some situations.
Another approach is the delivery of thrombolytic drugs like tPA or urokinase directly to the site of the blockage using a similar catheter. Clinical trials find it’s effective when used up to six hours after stroke. Many centers are using this procedure, although it requires experienced physicians and backup systems in case of complications.
Antiplatelet drugs prevent clotting by decreasing the activity of platelets (blood cells that help blood clot). These drugs reduce the risk of blood clots, thus reducing the risk of ischemic stroke. Health care professionals typically prescribe antiplatelet drugs after a stroke to prevent another one.
The most widely known and used antiplatelet drug is aspirin. Other antiplatelet drugs include clopidogrel (Plavix), ticlopidine (Ticlid), dipyridamole (Persantine) and Aggrenox, a combination of dipyridamole and aspirin. Anticoagulants reduce stroke risk by reducing the ability of the blood to clot. The most commonly used anticoagulants include warfarin (Coumadin) and heparin.
Researchers have conducted numerous studies to find out whether anticoagulants or antiplatelet drugs are better at preventing strokes. Several trials in patients with chronic atrial fibrillation, a common heart condition in which the heart rhythm is abnormal, find warfarin is best. But warfarin carries a risk of bleeding that requires careful monitoring of blood levels with regular blood tests. Aspirin is also a modestly effective therapy in atrial fibrillation.
For most people who have had a stroke but who don’t have atrial fibrillation, there’s no evidence that warfarin or other anticoagulants are any better than aspirin. This was clearly demonstrated in two government-sponsored studies, the Warfarin Aspirin Recurrent Stroke Study (WARSS) and the Warfarin Aspirin Symptomatic Intracranial Disease (WASID) trial, as well as in the European/Australian Stroke Prevention in Reversible Ischaemia Trial (ESPRIT).
At this point, the American Heart Association says people with atrial fibrillation at high risk for stroke should probably be treated with warfarin instead of aspirin unless there are reasons not to do so. In people under age 75 and at low risk for stroke, aspirin is the standard treatment.
Neuroprotective agents are being developed to protect the brain from secondary injury caused by stroke. If given quickly enough after a stroke, these drugs may help minimize the damage that results from brain cells being deprived of oxygen. Although no neuroprotectants are currently approved for use in stroke, many are being studied. There are several classes of neuroprotectants that show promise for future therapy, including antioxidants, glutamate antagonists, statins and anti-inflammatory agents.
Surgery
Surgery can be used in some situations to prevent stroke, to treat acute stroke or to repair blood vessel damage or malformations in and around the brain from a stroke. There are two main types of surgery for stroke prevention and treatment: carotid endarterectomy to prevent ischemic stroke, and surgery to remove or repair blood vessel malformations or aneurysms to prevent hemorrhagic stroke.
Carotid endarterectomy ( CEA ) is a surgical procedure in which a health care professional removes fatty deposits (plaque) from the inside of one of the carotid arteries. These arteries are located in the neck and provide the main supply of blood to the brain. This treatment aims at treating underlying atherosclerosis, characterized by the buildup of plaque on the inside of large arteries.
More recently, health care professionals have begun to use a procedure called carotid artery stenting, a procedure that involves the insertion of an expanding metal scaffold (stent) into the neck artery after it has been widened with balloon dilation, to reduce carotid artery blockages. This procedure is usually reserved for patients who have had a TIA or stroke but can’t undergo surgery. Some cardiologists are also exploring the use of drug-eluting stents for use in stroke prevention. While stenting has certain advantages, it is not risk-free; both bare-metal and drug-eluting stents carry some risk. Studies evaluating the proper role of stenting in stroke prevention are ongoing.
One useful surgical procedure for treatment of brain aneurysms that could lead to a hemorrhagic stroke is “clipping.” Clipping involves clamping off the aneurysm from the blood vessel, reducing the chance it will burst and bleed.
Another therapy is the detachable coil technique for the treatment of high-risk aneurysms. Small platinum coils are inserted through an artery in the groin and threaded through the arteries to the site of the aneurysm. The coils are carefully packed into the aneurysm, causing a blood clot to form inside the aneurysm, thus strengthening the artery walls of the aneurysm and reducing the risk of rupture. The coiling procedure may be enough to treat the aneurysm, but if it isn’t, the surgeon can clip the aneurysm and clamp it closed, reducing the risk of hemorrhage and death.
Treatment after a Stroke
The disability resulting from strokes is devastating to the stroke victim and family, but the good news is that therapies are available to help rehabilitate post-stroke patients with any of the following:
- speech problems
- motor activity, coordination and weakness issues
- vision problems
- hearing problems
- cognitive problems
- behavioral problems
- memory problems
- emotional problems
- paralysis or weakness
Physical therapy (PT) is the cornerstone of any rehabilitation process and should be started as soon as possible. A physical therapist uses training, exercises and physical manipulation to restore movement, balance and coordination. Through PT, the stroke patient works to relearn simple motor activities such as walking, sitting, standing, lying down and switching from one movement to another.
Occupational therapy (OT) focuses on creating independence in stroke victims. It involves exercise and training to help a stroke patient relearn everyday activities such as eating, drinking, swallowing, dressing, bathing, cooking, reading, writing and using the toilet.
Recent studies found that specific types of physical therapy, such as constraint-induced movement therapy ( CIMT ), can improve outcomes even when started months or more after stroke. In CIMT , the stroke patient’s strong hand is put in a sling to prevent its use, and the patient undergoes intensive therapy during which they are forced to use the weak hand. In the Extremity Constraint Induced Therapy Evaluation (EXCITE) randomized trial, patients undergoing this treatment had better outcomes and used the weak hand more than patients who received more standard therapy regimens. Since the study, CIMT has become increasingly popular.
The researcher who developed CIMT and conducted the EXCITE trial recently did a follow-up study on patients who had had a stroke an average of 4.5 years before receiving CIMT . The patients showed “large to very large” improvements in the use of their affected arms, illustrating that CIMT may work to improve the lives of stroke survivors years after they’ve suffered a stroke. CIMT remains controversial, however, because it is a very intensive type of rehabilitative therapy that may not be suitable for all patients, and it remains unclear whether the benefits are due to the intensity of the therapy or the specific program involved.
Speech and language problems arise when brain damage occurs in the language centers of the brain, located on the left side of the brain. But this doesn’t mean a stroke patient will never have a command of language again. Thanks to the brain’s ability to learn and change (called brain plasticity), other areas of the brain can learn to take over some lost functions.
Speech therapy can help a stroke victim relearn language and speaking skills or learn other forms of communication. Such therapy is also needed if the stroke victim has problems understanding speech or written words or has problems forming words.
With time and patience, a person who has had a stroke may be able to regain some, perhaps all, language and speaking abilities. Generally, the majority of recovery takes place within the first six months after the stroke, but it all depends on how quickly rehabilitation begins and the extent of brain damage.
New advances in imaging and rehabilitation find that the brain can compensate for function lost as a result of stroke. For example, a stroke patient who is unable to recognize faces may gradually come to recognize faces again, even though the part of the brain originally programmed to perform that function is still dead. The plasticity of the brain and its ability to “rewire” connections between brain cells means one part of the brain can change function and take up the function of a disabled part.
Stroke patients may also need psychological or psychiatric help. Depression, anxiety, frustration and anger are common post-stroke occurrences. Talk therapy, sometimes in conjunction with the appropriate medication, often helps alleviate some of the mental and emotional problems arising from the stroke. Sometimes it is also beneficial for family members to seek counseling.
Prevention
Many—perhaps most—strokes can be prevented. Therapies to prevent a first or recurrent stroke are based on treating your underlying risk factors for stroke or on preventing the widespread formation of blood clots that can cause ischemic stroke in anyone, regardless of risk factors.
Some people simply have a higher risk for stroke than others. Factors such as age, gender, race/ethnicity and family history of stroke can’t be changed. But you can control other risk factors, such as high blood pressure or cigarette smoking.
The most significant risk factors for stroke are high blood pressure, heart disease, diabetes and smoking. Others include heavy alcohol consumption, high blood cholesterol, illicit drug use and genetic or congenital conditions, particularly problems with blood vessels. If you have more than one risk factor, you have “amplification of risk.” This means that the multiple risk factors compound their destructive effects and create an overall risk greater than simply adding the individual risks together.
Atrial fibrillation, a heart rhythm disturbance that causes the small chambers of the heart to beat irregularly and allows blood clots to form, is another risk factor for stroke. With this condition, your doctor will likely prescribe a medication like warfarin (Coumadin) which “thins” the blood to prevent clots.
Cigarette smoking is one of the greatest risk factors for stroke. Smoking almost doubles your risk for ischemic stroke, independent of other risk factors. It is also responsible for more strokes in young adults than older adults. Smoking increases the risk of stroke by promoting atherosclerosis, a condition in which arteries harden after years of buildup of plaque, cholesterol and other debris in the bloodstream. Narrowed arteries can’t effectively deliver blood to the brain, raising the risk of stroke. Smoking also increases levels of blood-clotting factors and weakens blood vessels, so if a stroke occurs, the damage may be worse.
Your relative risk of stroke drops immediately after you stop smoking, and it may take only a few years for a former smoker’s risk to drop to the level of someone who never smoked. One of the most important things you can do to prevent stroke is to stop smoking.
Your risk of stroke also goes up if you take oral contraceptives and smoke. Talk with your health care professional to weigh the pros and cons of oral contraceptives as compared to other forms of birth control.
High alcohol consumption (more than two drinks per day) may reduce the number of blood platelets, interfering with blood clotting and thickness and increasing the risk of a hemorrhagic stroke. It is clear that heavy drinking or binge drinking can lead to a rebound effect after the alcohol leaves your body and your blood thickness and platelet levels skyrocket, increasing the risk for ischemic stroke.
If you drink, do so in moderation. This means no more than one drink per day for women, and no more than two drinks per day for men. One drink equals 12 ounces of beer, four ounces of wine, or one and a half ounces of 80-proof liquor. If you are a nondrinker, this is not a recommendation to start using alcohol. And certainly, if you are pregnant or have another health condition that could make alcohol use harmful, you should not drink.
The use of illicit drugs, such as cocaine, crack cocaine and amphetamines, can cause stroke. Cocaine can aggravate other risk factors, such as hypertension, heart disease and vascular disease, triggering a stroke. It decreases blood flow to the brain, causes blood vessels to tighten and prevents blood vessels from relaxing, leading to narrowing of the arteries. It also affects the heart, causing arrhythmias and rapid heart rates that can lead to blood clots.
Marijuana is sometimes identified as a risk because it reduces blood pressure and may interact with other risk factors, such as hypertension and cigarette smoking, to cause rapidly fluctuating blood pressure levels, damaging blood vessels. Other drugs of abuse, such as heroin and anabolic steroids—and even some over-the-counter diet aids—may increase stroke risk. Many of these drugs are vasoconstrictors, meaning that they may cause blood vessels to constrict and blood pressure to rise.
Diet may also be a factor. One study finds that eating five to six servings of fruits and vegetables a day can reduce the risk of ischemic stroke by a third compared to eating fewer vegetables and fruits. The American Heart Association recommends a healthy, balanced diet rich in fruits, vegetables, whole grains, and low-fat or fat-free dairy products.
So, here’s what you can do to reduce your risk of stroke:
- Stop smoking.
- Check your blood pressure regularly; if it is high, work with your health care professional to keep it under control. A normal blood pressure reading is less than 120/80.
- Restrict salt intake to reduce your blood pressure if you have high blood pressure.
- Find out if you have atrial fibrillation, or an irregular beating of the heart. This is a risk for blood clots. If you do have atrial fibrillation, your health care professional may prescribe a blood-thinning medication to prevent clots, depending on any other risk factors.
- Drink alcohol in moderation. Moderate drinking is defined as no more than one drink per day for women and no more than two for men. (A standard drink is one 12-ounce bottle of beer or wine cooler, one 4-ounce glass of wine, or 1.5 ounces of 80-proof distilled spirits.) This is intended to measure the amount consumed on a single day and does not represent an average over several days. In other words, if you don’t drink all week and then drink seven drinks on Saturday, it’s not the same as having one drink a day. More than a drink in a single day is considered heavy drinking in women.
- Have your cholesterol checked. Healthy cholesterol guidelines for individuals without heart disease are:
- total cholesterol levels less than 200 mg/dL
- HDL (high density lipoprotein) levels 50 mg/dL or higher for women; 40 mg/dL or higher for men.
- LDL (low-density lipoprotein)
- People who are at a low risk for heart disease: levels less than 160 mg/dL
- People who are at an intermediate risk for heart disease: levels less than 130 mg/dL
- People who are at a high risk for heart disease: levels less than 100 mg/dL
- People who are at a very high risk for heart disease: levels less than 70 mg/dL
- Triglycerides (another type of lipid) less than 150 mg/dL
For more information on blood cholesterol.
- If you have high blood cholesterol, discuss treatment options with your health care professional.
- If you have already had a stroke, ask your doctor whether you should be on a statin medicine. While these medications are generally used to lower cholesterol, there is strong evidence that they reduce the risk of stroke.
- If you have diabetes, work with your health care professional to control the disease.
- Exercise regularly.
- Treat any circulation problems.
Facts to Know
- Stroke, or brain attack, is the leading cause of serious disability in adults. Millions of Americans are living with the effects of stroke. About 10 percent recover completely; 25 percent recover with mild impairments; 40 percent are moderately to severely impaired, requiring special care; and the remainder require care in a nursing home or long-term care facility.
- You can have a stroke at any age; it strikes all age groups. More than 25 percent of stroke victims are under 65.
- Even though a stroke can occur at any age, the older you get, the greater your risk. For every decade after age 55, your risk of stroke increases 10 percent; two-thirds of all strokes occur in people over 65 years old.
- In 2004, 40 percent of those who died from stroke were men, and 60 percent were women.
- Race is a factor in stroke risk with blacks at greater risk than whites. In white women, the incidence of TIA and stroke is nearly 5 percent in women ages 55 to 64 and nearly 10 percent for ages 65 to 74. In black women, the incidence is 10 percent for ages 55 to 64 and 15 percent for ages 65 to 74. In white men, the incidence is about 6 percent for ages 55 to 64 and 12 percent for ages 65 to 74, and in black men the incidence is 13 percent for ages 55 to 64 and 16 percent for ages 65 to 74.
- There are two forms of stroke: ischemic (blockage of a blood vessel supplying the brain) and hemorrhagic (bleeding into or around the brain).
- People in the southeastern United States have the highest stroke mortality rate in the country. Researchers have dubbed this area the “stroke belt.” The buckle of the stroke belt—coastal North Carolina, South Carolina and Georgia—has a mortality rate higher than other parts of the belt and up to two times the stroke mortality rate than that of the United States overall. The increased risk could be due to geographic or environmental factors or to regional differences in lifestyle, including higher rates of cigarette smoking and a regional preference for salty, high-fat foods.
- The most important risk factors for stroke are hypertension, heart disease, diabetes and cigarette smoking. Other risks include heavy alcohol consumption, high blood-cholesterol levels, illicit drug use and genetic or congenital conditions (particularly vascular abnormalities). Having more than one risk factor amplifies risk.
- If you have the sudden onset of the worst headache of your life or the sudden onset of neurological symptoms, call 911 to get to a hospital immediately. A stroke must be diagnosed as either ischemic or hemorrhagic to determine the appropriate treatment, and some of those treatments have to be given within just several hours of the stroke’s onset. Time is of the essence.
- Pregnancy may increase the risk of stroke, particularly in pregnant women who experience complications, such as preeclampsia or postpartum hemorrhage. Severe headaches or visual changes after delivery can be a warning sign of blood clots in the brain’s venous drainage system and should be reported to your doctor immediately.
- Women with pregnancy complications may also be at longer term risk of stroke. A 2005 study published in the journal Obstetrics and Gynecology found that women with pregnancy complications were nearly 75 percent more likely to suffer a stroke in the 13.5 years following their pregnancies than women with no pregnancy complications.
- Dietary changes may reduce your risk. Reducing salt and fat intake can reduce your chances of developing high blood pressure and hardening of the arteries. There is also some evidence that boosting your intake of B vitamins may help reduce risk of stroke.
Key Q&A
- What is a stroke?A stroke or “brain attack” is caused by inadequate blood flow to the brain. It occurs when a blood clot blocks a blood vessel or artery, or when a blood vessel breaks, interrupting blood flow to an area of the brain.
- How can I prevent a stroke?You can’t always prevent a stroke, but many could be prevented by heeding stroke’s warning signs and treating its underlying risk factors, including high blood pressure, cigarette smoking, diabetes, high blood cholesterol and heart disease.
- What is most likely to put me at risk?Hypertension is the most important risk factor for stroke, increasing risk up to six times.
- What’s a “ministroke”?A transient ischemic attack (TIA), also known as a ministroke, is a brief episode of stroke symptoms caused by temporary interruptions of blood flow to the brain. A TIA starts just like a stroke but then resolves, leaving no noticeable symptoms or deficits. The average duration of a TIA is a few minutes, and most go away within an hour. Unlike actual strokes, TIAs do not kill brain cells, and therefore do not result in permanent neurological impairment. However, they can be important warning signs of an impending stroke. According to the American Heart Association, more than a third of people who have had a TIA will go on to have a stroke, and in half of those cases, the stroke will occur within a year of the TIA. Thus, the occurrence of a TIA should be taken very seriously, and medical attention should be sought immediately to prevent a disabling stroke.
- If it doesn’t kill me, I’ll get over a stroke, right?Not always. Stroke is the leading cause of serious adult disability. About 10 percent recover completely; 25 percent recover with mild impairments; 40 percent are moderately to severely impaired, requiring special care; and the remainder require care in a nursing home or long-term care facility.
- What’s the most common type of stroke?Ischemic strokes account for about 87 percent of all strokes. In these strokes, blood clots block an artery, depriving brain cells of oxygen.
- What are the psychological effects of a stroke?Depression, anxiety, frustration and anger are common post-stroke disabilities. Talk therapy, sometimes in conjunction with appropriate medication, can help alleviate some of the mental and emotional problems arising from the stroke. There is evidence that antidepressant medications given after stroke can prevent the development of depression in some patients. Sometimes it is also beneficial for family members to seek counseling.
- Are women at greater risk for a stroke?In 2006, women accounted for 60.2 percent of stroke deaths. And of every10 deaths from stroke, four occur in men and six occur in women. This is because the average life expectancy for women is greater than for men, and the highest rates for stroke are in the oldest age groups . Moreover, pregnancy, childbirth (particularly the postpartum period) and menopause are added risk factors.
- What are the symptoms of a stroke?Primary symptoms include sudden numbness or weakness, especially on one side of the body; sudden confusion or trouble speaking or understanding speech; sudden trouble seeing out of one or both eyes; sudden trouble walking, dizziness or loss of balance or coordination; or sudden severe headache with no known cause.
- What should I do if I think I might be having a stroke?Call 911 to get to a hospital immediately. Thrombolytic agents, or clot busters, are effective at treating ischemic strokes (the most common kind), but they must be administered within three hours of the onset of a stroke. They can only be given, however, after your health care professional has confirmed that the stroke is ischemic, not hemorrhagic. Hence, time is of the essence.
- Do I have atrial fibrillation, and what can I do to test my pulse for the development of this condition?Atrial fibrillation is a heart rhythm disturbance that causes the small chambers of the heart to beat irregularly, allowing blood clots to form. About 15 percent of strokes occur in people with atrial fibrillation. It is particularly common in older people; three to five percent of people over 65 have the condition. It may also occur in younger women, particularly in association with hyperthyroidism or Graves’ disease. Your health care professional can tell you whether or not you have atrial fibrillation just by checking your pulse. By learning to check for it yourself, you can periodically monitor yourself to rule out this important cause of stroke. It is important to recognize atrial fibrillation because strokes can be prevented by using a blood thinning medication to prevent clots from forming in the heart.
For more information visit us our website: https://www.healthinfi.com
0 200

No Comments