Chronic Lymphocytic Leukemia (CLL)
Overview
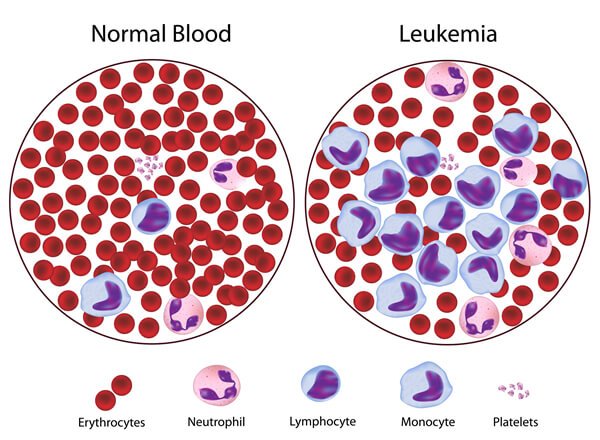
Chronic lymphocytic leukemia (CLL) is a type of cancer of the blood and bone marrow — the spongy tissue inside bones where blood cells are made. The term “chronic” in chronic lymphocytic leukemia comes from the fact that it typically progresses more slowly than other types of leukemia. The term “lymphocytic” in chronic lymphocytic leukemia comes from the cells affected by the disease — a group of white blood cells called lymphocytes, which help your body fight infection. Chronic lymphocytic leukemia (CLL) is a cancer that affects a type of white blood cell called a “lymphocyte.” Lymphocytes help your body fight infection. They’re made in the soft center of your bones, called the marrow. If you have CLL, your body makes an abnormally high number of lymphocytes that aren’t working right.
Chronic lymphocytic leukemia most commonly affects older adults. There are treatments to help control the disease. Chronic lymphocytic leukaemia (CLL) is a kind of moderate developing leukemia that influences creating B-lymphocytes. B lymphocytes (otherwise called B-cells) are specific white platelets. Under ordinary conditions they create immunoglobulins (likewise called antibodies) that assistance ensure our bodies against contamination and malady. In individuals with CLL, lymphocytes experience a harmful (destructive) change and move toward becoming leukaemic cells.
It is critical to accentuate that for some individuals CLL stays stable for a long time and years and has pretty much nothing, assuming any, affect on their way of life or general wellbeing. Around 30-half of individuals determined to have CLL never require any treatment for their infection and can make due for a long time in spite of their finding. For others, the leukaemic cells increase in an uncontrolled way, live longer than they should and amass in the bone marrow, circulatory system, lymph hubs (organs), spleen, liver and different parts of the body. These cells are strange and all things considered can’t work legitimately. After some time, an abundance number of lymphocytes swarm the bone marrow, and meddle with ordinary platelet generation.
CLL ordinarily grows gradually and advances gradually, finished months and years. The vast majority have no indications of their ailment when initially analyzed. In these cases, individuals frequently require no treatment for quite a while, aside from consistent registration with their specialist to deliberately screen their wellbeing. Others may should be dealt with not long after they are analyzed. More adults get CLL than any other type of leukemia. It usually grows slowly, so you may not have symptoms for years.
Some people never need treatment, but if you do, it can slow the disease and ease symptoms. People who get medical care live longer today, because doctors are diagnosing CLL earlier.
It’s natural to have worries and questions about any serious condition. You don’t have to face things alone. Tell your friends and family about any concerns you have. Let them know how they can help. And talk to your doctor about how to join a support group. It can help to speak to people who understand what you’re going through.
Symptoms
Many people with chronic lymphocytic leukemia have no early symptoms. Those who do develop signs and symptoms may experience:
- Enlarged, but painless, lymph nodes
- Fatigue
- Fever
- Pain in the upper left portion of the abdomen, which may be caused by an enlarged spleen
- Night sweats
- Weight loss
- Frequent infections
Patients with CLL give an extensive variety of manifestations and signs. Beginning is deceptive, and it isn’t abnormal for CLL to be found unexpectedly after a platelet tally is performed for another reason; 25-half of patients will be asymptomatic at time of introduction.Enlarged lymph nodes, liver, or spleen
- Recurring infections
- Loss of appetite or early satiety
- Abnormal bruising (late-stage symptom)
- Fatigue
- Night sweats
Causes
The exact cause of most cases of chronic lymphocytic leukemia (CLL) is not known. But scientists have learned a great deal about the differences between normal lymphocytes and CLL cells in recent years.
Typical human cells develop and work construct for the most part with respect to the data contained in every cell’s chromosomes. Chromosomes are long atoms of DNA. DNA is the synthetic that conveys our qualities – the directions for how our cells work. We resemble our folks since they are the wellspring of our DNA. Be that as it may, our qualities influence more than the way we look. Each time a cell gets ready to isolate into 2 new cells, it must make another duplicate of the DNA in its chromosomes. This procedure isn’t immaculate, and blunders can happen that may influence qualities inside the DNA.
A few qualities contain directions for controlling when our cells develop and separate. Certain qualities that advance cell development and division are called oncogenes. Others that back off cell division or make cells kick the bucket at the correct time are called tumor silencer qualities. Diseases can be caused by DNA transformations (changes) that turn on oncogenes or kill tumor silencer qualities.
Every human cell contains 23 sets of chromosomes. Much of the time of CLL, a change can be found in no less than one of these chromosomes. Frequently this change is a cancellation − that is, loss of part of a chromosome. The loss of part of chromosome 13 is the most well-known erasure, yet different chromosomes, for example, 11 and 17 can likewise be influenced. In some cases there is an additional chromosome 12 (trisomy 12). Other, less normal irregularities may likewise be found. Researchers know these chromosome changes are critical in CLL, however it’s not yet clear which qualities they include or precisely how they prompt leukemia.
We do realize that typical B lymphocytes are a piece of the insusceptible framework. They are modified to develop and isolate when they come into contact with an outside substance called an antigen. (Researchers call substances remote on the off chance that they don’t regularly happen in a man’s body and can be perceived by their safe framework. Germs contain outside antigens. So do platelets from another person with an alternate blood classification.) Researchers feel that CLL starts when B lymphocytes keep on dividing without restriction after they have responded to an antigen. Be that as it may, why this happens isn’t yet known.
Now and then individuals acquire DNA changes from a parent that significantly increment their danger of getting certain kinds of growth. Yet, acquired changes once in a while cause CLL. DNA changes identified with CLL as a rule happen amid the individual’s lifetime, as opposed to having been acquired before birth.
Doctors aren’t certain what starts the process that causes chronic lymphocytic leukemia. What’s known is that something happens to cause a genetic mutation in the DNA of blood-producing cells. This mutation causes the blood cells to produce abnormal, ineffective lymphocytes. Beyond being ineffective, these abnormal lymphocytes continue to live and multiply, when normal lymphocytes would die. The abnormal lymphocytes accumulate in the blood and certain organs, where they cause complications. They may crowd healthy cells out of the bone marrow and interfere with normal blood cell production. Doctors and researchers are working to understand the exact mechanism that causes chronic lymphocytic leukemia.
- You have a parent, sibling, or child who has CLL.
- You’re middle-aged or older.
- You’re a white man.
- You have relatives who are either Eastern European or Russian Jews.
- If you were exposed to Agent Orange, an herbicide widely used during the Vietnam War, your chances of getting CLL may also be higher.
Risk factors
Factors that may increase the risk of chronic lymphocytic leukemia include:
- Your age.This disease occurs most often in older adults. On average, people diagnosed with chronic lymphocytic leukemia are in their 70s.
- Your race.Whites are more likely to develop chronic lymphocytic leukemia than are people of other races.
- Family history of blood and bone marrow cancers.A family history of chronic lymphocytic leukemia or other blood and bone marrow cancers may increase your risk.
- Exposure to chemicals.Certain herbicides and insecticides, including Agent Orange used during the Vietnam War, have been linked to an increased risk of chronic lymphocytic leukemia.
Doctors don’t know why some cells become leukemic cells and others don’t. For most people who have chronic lymphocytic leukemia (CLL), there are no obvious reasons why they developed the disease.
- CLL has generally not been associated with any environmental or external risk factors with one exception (see “A Risk for Vietnam Veterans,” below).
- Researchers have concluded that there’s no way to prevent CLL.
- You can’t catch CLL from someone else.
- Experts have found that in a small number of cases, first-degree relatives (parents and siblings) of people with CLL are three to four times more likely to develop CLL than people who don’t have first-degree relatives with the disease. But the link isn’t common, and the risk is small.
A Risk for Vietnam Veterans
Researchers have found a potential association between CLL and exposure to herbicides like Agent Orange used during the Vietnam conflict from 1961 to 1971. The U.S. Department of Veterans Affairs (VA) entitles those exposed to receive disability compensation. If you have CLL and think you may have been exposed to Agent Orange or other herbicides, you’re entitled to benefits. The VA is urging Vietnam veterans to apply for compensation to begin processing their claims.
Diagnosis
Patients with CLL have a higher-than-normal white blood cell count, which is determined by complete blood count (CBC). Peripheral blood flow cytometry is the most valuable test to confirm a diagnosis of CLL. Other tests that may be helpful for diagnosis include bone marrow biopsy and ultrasonography of the liver and spleen. Immunoglobulin testing may be indicated for patients developing repeated infections.
Staging
Two staging systems are used for CLL.
The Rai-Sawitsky staging system categorizes patients into low-, intermediate-, and high-risk groups, as follows:
- Low risk (formerly stage 0) – Lymphocytosis in the blood and marrow only (25% of presenting population)
- Intermediate risk (formerly stages I and II) – Lymphocytosis with enlarged nodes in any site or splenomegaly or hepatomegaly (50% of presentation)
- High risk (formerly stages III and IV) – Lymphocytosis with disease-related anemia (hemoglobin < 11 g/dL) or thrombocytopenia (platelets < 100 x 10 9/L) (25% of all patients) The Binet staging system categorizes patients according to the number of lymph node groups involved, as follows:
- Stage A – Hemoglobin 10 g/dL or higher, platelets 100 × 10 9/L or higher, and fewer than three lymph node areas involved.
- Stage B – Hemoglobin and platelet levels as in stage A and three or more lymph node areas involved
- Stage C – Hemoglobin less than 10 g/dL or platelets less than 100 × 10 9/L, or both.
Treatment
Your treatment options for chronic lymphocytic leukemia depend on several factors, such as the stage of your cancer, whether you’re experiencing signs and symptoms, your overall health, and your preferences.
Chemotherapy. You may get this by pill, shot, or IV. Doctors often combine two or more drugs that work in different ways to kill the cancer cells.
Immunotherapy. These drugs prompt your body’s immune system to recognize and destroy cancer cells. You often get it along with chemotherapy.
Radiation therapy. This type of treatment uses high-energy rays, such as X-rays, to destroy cancer cells. You probably won’t need it, unless your doctor recommends it to shrink swelling in a lymph node, in your spleen, or in another organ that’s causing pain.
Treatment may not be necessary in early stages
People with early-stage chronic lymphocytic leukemia typically don’t receive treatment. Studies have shown that early treatment doesn’t extend lives for people with early-stage chronic lymphocytic leukemia. Rather than put you through the potential side effects and complications of treatment before you need it, doctors carefully monitor your condition and reserve treatment for when your leukemia progresses. Doctors call this watchful waiting.
Your doctor will plan a checkup schedule for you. You may meet with your doctor and have your blood tested every few months to monitor your condition. Treatment for people with early-stage chronic lymphocytic leukemia is offered only through clinical trials. Studies that evaluate whether early treatment may be helpful might be an option for people with early-stage disease that has a high risk of progression. Talk to your doctor about your options.
Treatments for intermediate and advanced stages
Your doctor uses the stage of your chronic lymphocytic leukemia, results from various tests —including laboratory analysis of your cancer cells — and your overall health to make recommendations about your treatment.
If your doctor determines your chronic lymphocytic leukemia is progressing or is in the intermediate or advanced stages, your treatment options may include:
- Chemotherapy is a drug treatment that kills quickly growing cells, including cancer cells. Chemotherapy treatments can be administered through a vein or taken in pill form. Depending on your situation, your doctor may use a single chemotherapy drug or you may receive a combination of drugs.
- Targeted drug therapy.Targeted drugs are designed to take advantage of the specific vulnerabilities of your cancer cells. Your cancer cells are tested to determine which targeted drugs may be helpful.
- Immunotherapy is a treatment that uses your body’s immune system to fight cancer. Immunotherapy treatments may make it easier for your immune system to identify cancer cells or train your immune system cells to fight cancer cells.
- Bone marrow transplant.A bone marrow transplant, also known as a stem cell transplant, uses strong chemotherapy drugs to kill the stem cells in your bone marrow that are creating diseased lymphocytes. Then healthy adult blood stem cells from a donor are infused into your blood, where they travel to your bone marrow and begin making healthy blood cells.
As new and more-effective drug combinations have been developed, bone marrow transplant has become less common in treating chronic lymphocytic leukemia. Still in certain cases, this may be a treatment option.
For More Information Visit Us Our Website: https://www.healthinfi.com
0 200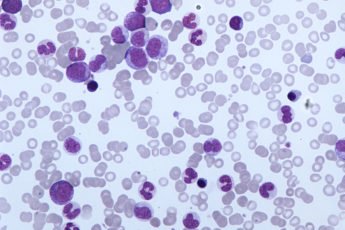
No Comments