
Acanthotic nevus
Acanthotic nevus is an alternate name for seborrheic keratosis. It is a rare skin disease that consists of discolored lesions that appear to be oily. Since these lesions seem to be stuck on the epidermis, they are sometimes mistaken for cancerous growths. Acanthotic nevus develops usually on people who are above the age of 40. Among the symptoms of this disease is itching, swelling of lesions as well as irritability. Surgical treatment may be needed to remove the lesions.
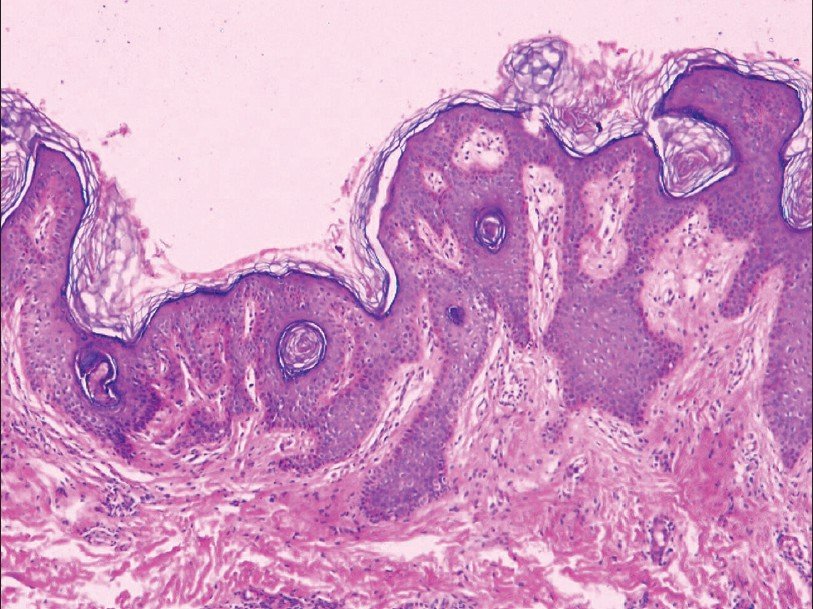
Histology of epidermal naevus
The scanning power view of epidermal naevus is of an epidermal proliferative process Low power reveals hyperkeratosis and papillomatosis across the breadth of the specimen.Epidermal hyperplasia forms finger like projections with the intervening invaginations filled with hyperkeratotic material. Frequently incidental fungal spore forms are seen. Extending below the projections into the dermis are anastamosing thickened cords of acanthotic epidermis. Dermal collagen and telangiectatic vessels can be seen within the papillary projections .
A variable inflammatory infiltrate may accompany the epidermal changes, more prominent in the inflammatory verrucous variant.
Histological variants of epidermal naevus
A number of reported variants exist including acantholytic, porokeratotic, acanthosis nigricans like, Hailey-Hailey disease-like and verrucous.
Differential diagnosis of epidermal naevus
Inflammatory Verrucous Epidermal Naevus (ILVEN): This naevus is likely simply a subtype of the epidermal naevus. In addition to the superficial perivascular or lichenoid lymphocytic infiltrate specific epidermal changes are recognised. Areas of alternating parakeratosis and orthokeratosis are seen. Beneath the parakeratosis there is hypogranulosis, whereas beneath the orthokeratosis there is hypergranulosis.
Seborrhoeic keratosis: While clinical correlation is essential here, the presence of elongated down-growths of epidermis with some flattening at the base is more in keeping with an epidermal nevus.
Abstract
Eight cases of the acanthosis nigricans form of epidermal nevus have been described in literature. The present case is impressive and has an extensive segmental distribution. Although etiological factors, such as mutations in the FGFR3 gene, are becoming recognized, treatment options remain limited. We present a case of a 14-year-old male with multiple hyperpigmented, hyperkeratotic plaques on the upper body, axillae, and groin with a segmental distribution following Blaschko lines. Histopathological investigation showed aspects of both acanthosis nigricans and epidermal nevus. So far, screening has not revealed any internal abnormalities. As previous cases show a clear association with internal diseases, repetitive screening for internal diseases and syndromes is suggested in the case of the acanthosis nigricans form of epidermal nevus. Treatment of the condition remains a challenge.
Acanthosis nigricans (AN) is usually a symmetric eruption characterized by a hyperpigmented, velvety cutaneous thickening that can occur on any part of the body, but characteristically affects the axillae, nape and the sides of the neck, the groin, antecubital and popliteal surfaces, and umbilical area. t is a cutaneous marker, most frequently of insulin resistance and less frequently of malignancy. [2] Nevoid AN is a rare form of AN that manifests at any age at or before puberty and has a morphologic pattern similar to other forms of AN.It is not associated with syndromes, endrocrinopathies, drugs, or malignancies.It is said to be inherited as an irregularly autosomal dominant trait that may first become evident at birth, in childhood, or during puberty. Nevoid AN classically extends for a certain period and then either remains stationary or starts regressing. enign AN and benign inherited AN, are the names proposed by some authors for the same disorder. Unilateral nevoid AN is another term that has also been used to denote this entity. A case of nevoid AN is reported here as the condition was rarely reported from India and in world literature.
An 18-year-old girl presented with a localized area of nonpruritic thickened and pigmented skin on right side of the nape of the neck for 7 years. The first-born among three children born to nonconsanguineous parents, she did not have any other member of her family affected with similar lesions [Figure 1]. It started as a small brown asymptomatic papule a little behind the right ear, and gradually spread to the present size in a span of 3 years, and then stopped growing further. There was no history of rubbing the area. On dermatological examination, a brown black velvety plaque with soft ridges, measuring about 7 cm ´ 5 cm, was seen. The borders were irregular with the affected skin gradually merging imperceptibly with normal skin. The skin was otherwise normal. Palms and soles, mucous membranes, genitals, hair, and nails were normal. The patient was non-obese, with a body mass index (BMI) of 20.1, and systemic examination was unremarkable. Complete blood count and routine urine analysis were within normal limits. Venereal Disease Research Laboratory (VDRL) test was nonreactive. Fasting blood sugar was 87 mg/dl and postprandial blood sugar was 108 mg/dl. Fasting insulin level was 11.3 IU/ml.
The hepatic enzymes, T3, T4, TSH, and growth hormone were within normal range. Radiographic examination of the chest, skull, and hands were normal. Abdominal ultrasonography was normal. Biopsy of the skin showed hyperkeratosis, papillomatosis, increased pigmentation of the basal cell layer, and mild acanthosis, with a sparse inflammatory infiltrate of mononuclear cells in the upper dermis.
Nevoid AN has been grouped together with “syndromic AN” and “acral acanthotic anomaly” under the heading “other” causes of AN in a recent classification of AN. Nevoid AN is said to have resemblance to ichthyosis hystrix and confluent reticulate papillomatosis, but in this case they could be clinically ruled out. Differentiation from linear epidermal nevus and from the hyperkeratotic type of seborrheic keratosis is more difficult, and it has even been suggested that this form of AN can be classified as a type of epidermal nevus so far as the histogenesis of this lesion is concerned, although its status as a distinct clinical and histopathological entity is recognized.However, in this case seborrheic keratosis could be ruled out clinically. Linear epidermal nevus, which shows more marked acanthosis and has a more compact orthokeratotic stratum corneum, was ruled out histologically. In view of the fact that nevoid AN is considered an irregularly autosomal dominant trait, the absence of family history is noteworthy.
Important
It is possible that the main title of the report Keratosis, Seborrheic is not the name you expected. Please check the synonyms listing to find the alternate name(s) and disorder subdivision(s) covered by this report.
Synonyms
- Acanthotic Nevus
- Keratosis Seborrheica
- Seborrheic Warts
- Senile Warts
- Verruca
- Disorder Subdivisions
- None
- General Discussion
Seborrheic Keratosis is a skin disorder usually characterized by discolored lesions that appear to be “stuck on” the skin surface. Warts may appear and skin is often oily or greasy. These skin lesions are sometimes mistaken for cancerous growths and tend to appear predominately during middle age. Itching, irritation, inflammations or unsightliness of lesions may require surgical removal of affected skin areas.
Diagnostic Considerations
The clinical differential diagnosis of seborrheic keratoses includes malignant melanoma, melanocytic nevus, verruca vulgaris, condyloma acuminatum, fibroepithelial polyp, epidermal nevus, actinic keratoses, pigmented basal cell carcinomas, and squamous cell carcinomas.
Melanoma can clinically resemble seborrheic keratosis. A retrospective review of 9204 consecutive pathology reports from the Massachusetts General Hospital containing a clinical diagnosis of seborrheic keratosis revealed that 61 of these specimens (0.66%) were malignant melanoma. The submitted clinical differential diagnosis was seborrheic keratosis versus melanoma (31 cases, 51%), melanocytic nevus (17 cases, 28%), basal cell carcinoma (7 cases, 12%), squamous proliferation (3 cases, 5%), and no other differential diagnosis (3 cases, 5%).
Distinguishing superficial seborrheic keratoses from lentigo maligna and pigmented actinic keratoses may be difficult. The pigmented domed variety of acanthotic seborrheic keratoses may closely resemble a melanocytic nevus, but the surface is less lustrous and the follicular orifices are plugged.
Some seborrheic keratoses have a verrucous architecture that can produce a clinical and histologic appearance similar to an aging viral wart. Routine histopathologic examination may not reliably make this distinction, and special studies to look for evidence of papillomavirus DNA may be needed.
Differential Diagnoses
- Acrochordon
- Acrokeratosis Verruciformis of Hopf
- Actinic Keratosis
- Arsenical Keratosis
- Basal Cell Carcinoma
- Bowen Disease
- Bowenoid Papulosis
- Confluent and Reticulated Papillomatosis
- Cutaneous Horn
- Cutaneous Manifestations of HIV
- Cutaneous Melanoma
- Cutaneous Squamous Cell Carcinoma
- Dermatosis Papulosa Nigra
- Epidermal Nevus Syndrome
- Epidermodysplasia Verruciformis
- Erythroplasia of Queyrat (Bowen Disease of the Glans Penis)
- Genital Warts
- Guttate Psoriasis
- Lentigo
- Melanocytic Nevi
- Nevus Sebaceus
- Nongenital Warts
- Pemphigus Erythematosus
- Plaque Psoriasis
- Premalignant Fibroepithelial Tumor (Pinkus Tumor)
- Prurigo Nodularis
- Sign of Leser-Trelat
- Stucco Keratosis
The epidermal nevus is a non-cancerous hamartoma or skin lesion found on the outer portion of the skin. They are caused by an overgrowth of cells in the epidermis and usually appear at birth or in early childhood. Epidermal nevi are fairly common congenital malformations that occur in 1-3 per 1000 births and are asymptomatic.
For more information visit us our website: https://www.healthinfi.com
0 200
1 Comment