Appendicitis
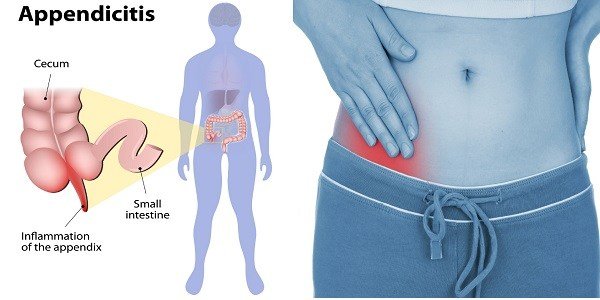
Appendicitis is an inflammation of the appendix, a 3 1/2-inch-long tube of tissue that extends from the large intestine. One study suggests that the appendix may have some role in gut immunity, but nothing is definite. One thing we do know: We can live without it, without apparent consequences.
Appendicitis is a medical emergency that almost always requires prompt surgery to remove the appendix. Left untreated, an inflamed appendix will eventually burst, or perforate, spilling infectious materials into the abdominal cavity. This can lead to peritonitis, a serious inflammation of the abdominal cavity’s lining (the peritoneum) that can be fatal unless it is treated quickly with strong antibiotics
Sometimes a pus-filled abscess (infection that is walled off from the rest of the body) forms outside the inflamed appendix. Scar tissue then “walls off” the appendix from the rest of the abdomen, preventing infection from spreading. An abscessed appendix can perforate or explode and cause peritonitis. For this reason, almost all cases of appendicitis are treated as emergencies, requiring surgery.
In the U.S., one in 20 people will get appendicitis. Although it can strike at any age, appendicitis is rare under age 2 and most common between ages 10 and 30. Appendicitis occurs when the appendix becomes blocked, often by stool, a foreign body, or cancer. Blockage may also occur from infection, since the appendix can swell in response to any infection in the body.
Appendicitis is an inflammation of the appendix, a finger-shaped pouch that projects from your colon on the lower right side of your abdomen. The appendix doesn’t seem to have a specific purpose. Appendicitis causes pain in your lower right abdomen. However, in most people, pain begins around the navel and then moves. As inflammation worsens, appendicitis pain typically increases and eventually becomes severe.
Although anyone can develop appendicitis, most often it occurs in people between the ages of 10 and 30. Standard treatment is surgical removal of the appendix.
Symptoms
The classic symptoms of appendicitis include:
- Dull pain near the navel or the upper abdomen that becomes sharp as it moves to the lower right abdomen. This is usually the first sign.
- Loss of appetite
- Nausea and/or vomiting soon after abdominal pain begins
- Abdominal swelling
- Fever of 99-102 degrees Fahrenheit
- Inability to pass gas
Almost half the time, other symptoms of appendicitis appear, including:
- Dull or sharp pain anywhere in the upper or lower abdomen, back, or rectum
- Painful urination and difficulty passing urine
- Vomiting that precedes the abdominal pain
- Severe cramps
- Constipation or diarrhea with gas
If you have any of the mentioned symptoms, seek medical attention immediately, because timely diagnosis and treatment is very important. Do not eat, drink, or use any pain remedies, antacids, laxatives, or heating pads, which can cause an inflamed appendix to rupture.
The presentation of acute appendicitis includes abdominal pain, nausea, vomiting, and fever. As the appendix becomes more swollen and inflamed, it begins to irritate the adjoining abdominal wall. This leads to the localization of the pain to the right lower quadrant. This classic migration of pain may not be seen in children under three years. This pain can be elicited through signs and can be severe. Signs include localized findings in the right iliac fossa.
The abdominal wall becomes very sensitive to gentle pressure (palpation). There is severe pain on sudden release of deep pressure in the lower abdomen (rebound tenderness). If the appendix is retrocecal (localized behind the cecum), even deep pressure in the right lower quadrant may fail to elicit tenderness (silent appendix). This is because the cecum, distended with gas, protects the inflamed appendix from pressure. Similarly, if the appendix lies entirely within the pelvis, there is usually complete absence of abdominal rigidity. In such cases, a digital rectal examination elicits tenderness in the rectovesical pouch. Coughing causes point tenderness in this area (McBurney’s point), historically called Dunphy’s sign.
Appendicitis typically begins with a vague pain in the middle of the abdomen often near the navel or “belly button” (umbilicus). The pain slowly moves to the right lower abdomen (toward the right hip) over the next 24 hours. In the classic description, abdominal pain may be accompanied with nausea, vomiting, lack of appetite, and fever. Fewer than half of people who develop appendicitis have all the symptoms. More commonly, people with appendicitis have any combination of these symptoms.
Symptoms of appendicitis may take 4 to 48 hours to develop. During this time, a person may have varying degrees of loss of appetite, vomiting, and abdominal pain. The person may have constipation or diarrhea, or there may be no change in bowel habits.
Early symptoms are often hard to separate from other conditions including gastroenteritis (an inflammation of the stomach and intestines). Many people admitted to the hospital for suspected appendicitis leave the hospital with a diagnosis of gastroenteritis; initially, true appendicitis is often misdiagnosed as gastroenteritis. Children and the elderly often have fewer symptoms, or cannot adequately describe their symptoms, which makes their diagnosis less obvious and the incidence of complications more frequent.
Most people with appendicitis have classic symptoms that a doctor can easily identify. The main symptom of appendicitis is abdominal pain. The abdominal pain usually
- occurs suddenly, often causing a person to wake up at night
- occurs before other symptoms
- begins near the belly button and then moves lower and to the right
- is new and unlike any pain felt before
- gets worse in a matter of hours
- gets worse when moving around, taking deep breaths, coughing, or sneezing
Other symptoms of appendicitis may include
- loss of appetite
- nausea
- vomiting
- constipation or diarrhea
- inability to pass gas
- a low-grade fever that follows other symptoms
- abdominal swelling
- the feeling that passing stool will relieve discomfort
Early signs and symptoms of appendicitis often are mild, consisting merely of a loss of appetite and/or nausea and a sense of not feeling well. There may not be even abdominal pain.
Nevertheless, as the course of the appendicitis progresses the main symptom becomes abdominal pain.
The pain is at first diffuse and poorly localized, that is, not confined to one spot. (Poorly localized pain is typical whenever a problem is confined to the small intestine or colon, including the appendix.) The pain is so difficult to pinpoint that when asked to point to the area of the pain, most people indicate the location of the pain with a circular motion of their hand around the central part of their abdomen.
With time, the pain may localize to the right lower abdomen, and the patient may be able to identify an exact location of the pain.
If not already present, a second symptom of appendicitis is loss of appetite which may progress to nausea and even vomiting. Nausea and vomiting also may occur later due to intestinal obstruction from the expanding inflammatory mass or abscess rather than from local inflammation.
As appendiceal inflammation increases, it may extend through the appendix to its outer covering and then to the lining of the abdomen, a thin membrane called the peritoneum. Once the peritoneum becomes inflamed, the character of the pain changes and then can be localized clearly to one small area. Generally, this area is between the front of the right hip bone and the belly button. The exact point is named after Dr. Charles McBurney-McBurney’s point. If the appendix ruptures and infection spreads throughout the abdomen, the pain becomes diffuse again as the entire lining of the abdomen becomes inflamed.
Signs and symptoms of appendicitis may include:
- Sudden pain that begins on the right side of the lower abdomen
- Sudden pain that begins around your navel and often shifts to your lower right abdomen
- Pain that worsens if you cough, walk or make other jarring movements
- Nausea and vomiting
- Loss of appetite
- Low-grade fever that may worsen as the illness progresses
- Constipation or diarrhea
- Abdominal bloating
The site of your pain may vary, depending on your age and the position of your appendix. When you’re pregnant, the pain may seem to come from your upper abdomen because your appendix is higher during pregnancy
How Is Appendicitis Diagnosed?
Diagnosing appendicitis can be tricky. Symptoms of appendicitis are frequently vague or extremely similar to other ailments, including gallbladder problems, bladder or urinary tract infection, Crohn’s disease, gastritis, intestinal infection, and ovary problems.
The following tests are usually used to help make the diagnosis:
- Abdominal exam to detect inflammation
- Urine test to rule out a urinary tract infection
- Rectal exam
- Blood test to see if your body is fighting infection
- CT scans and/or ultrasound
Appendicitis is diagnosed by the classic symptoms of appendicitis and physical examination (the doctor’s examination of the patient’s abdomen)
Lab work: Although no blood test can confirm appendicitis, a blood sample is sent for laboratory analysis to check the white blood cell count, which is typically elevated in an individual with appendicitis. However, normal levels can be present with appendicitis, and elevated levels can be seen with other conditions. A urinalysis may be ordered to exclude urinary tract infection (or pregnancy) as the cause of the patient’s symptoms.
Imaging tests: Imaging tests are ordered when the diagnosis is not readily apparent. A CT scan of the abdomen and pelvis can assist in evaluating abdominal pain suspected of being caused by appendicitis. Ultrasound scanning is commonly used in small children to test for appendicitis to avoid exposing the child to radiation from CT scans.
Other conditions that cause abdominal pain may mimic the symptoms of appendicitis making the diagnosis more difficult. These conditions include kidney stones, urinary tract infections, hernias, gallstones and gallbladder problems, colitis, diverticulitis, and ovarian or testicular problems.
The diagnosis of appendicitis begins with a thorough history and physical examination. Patients often have an elevated temperature, and there usually will be moderate to severe tenderness in the right lower abdomen when the doctor pushes there. If inflammation has spread to the peritoneum, there is frequently rebound tenderness. Rebound tenderness is pain that is worse when the doctor quickly releases his or her hand after gently pressing on the abdomen over the area of tenderness.
Diagnosis is based on a medical history (symptoms) and physical examination which can be supported by an elevation of neutrophilic white blood cells and imaging studies if needed. (Neutrophils are the primary white blood cells that respond to a bacterial infection.) Histories fall into two categories, typical and atypical.
Typical appendicitis includes several hours of generalized abdominal pain that begins in the region of the umbilicus with associated anorexia, nausea, or vomiting. The pain then “localizes” into the right lower quadrant where the tenderness increases in intensity. It is possible the pain could localize to the left lower quadrant in people with situs inversus totalis. The combination of pain, anorexia, leukocytosis, and fever is classic.
Atypical histories lack this typical progression and may include pain in the right lower quadrant as an initial symptom. Irritation of the peritoneum (inside lining of the abdominal wall) can lead to increased pain on movement, or jolting, for example going over speedbumps.[31] Atypical histories often require imaging with ultrasound or CT scanning.[32]
How Is Appendicitis Treated?
Surgery to remove the appendix, which is called an appendectomy, is the standard treatment for almost all cases of appendicitis.
Generally, if appendicitis is suspected, doctors tend to err on the side of safety and quickly remove the appendix to avoid its rupture. If the appendix has formed an abscess, you may have two procedures: one to drain the abscess of pus and fluid, and a later one to remove the appendix. However, there is some research showing that treatment of acute appendicitis with antibiotics may eliminate the need for surgery in certain cases.
Appendicitis can not be treated at home. If you suspect you have appendicitis, see your doctor or go to an emergency department. Treatment for appendicitis varies. In most cases, however, surgery will be necessary. The type of surgery will depend on the details of your case.
If you have an abscess that hasn’t ruptured, your doctor may first administer antibiotics. Your doctor will then drain the abscess using a tube placed through your skin. After you’ve received treatment for the infection, you’ll undergo surgery to remove your appendix.
If you have a ruptured abscess or appendix, surgery may be necessary right away. Surgery to remove the appendix is known as an appendectomy.
Your doctor can perform this procedure as open surgery or through a laparoscopy. Laparoscopy is less invasive, making the recovery time shorter. However, open surgery may be necessary if you have an abscess or peritonitis.
In rare cases, appendicitis may get better without surgery. This is only an option if your abdominal pain is minimal and your diagnostic tests are normal. In this scenario, your treatment plan might only involve antibiotics and a liquid diet until your symptoms resolve.
Causes
There is no clear cause of appendicitis. Fecal material is thought to be one possible cause of obstruction of the appendix. Bacteria, viruses, fungi, and parasites can result in infection, leading to the swelling of the tissues of the appendix wall. The various infecting organisms include Yersinia species, adenovirus, cytomegalovirus, actinomycosis, Mycobacteria species, Histoplasma species, Schistosoma species, pinworms, and Strongyloides stercoralis. Swelling of the tissue from inflammatory bowel disease such as Crohn’s disease also may cause appendicitis.
Appendicitis is not a hereditary disease and is not transmittable from person to person.
Appendicitis means inflammation of the appendix. It is thought that appendicitis begins when the opening from the appendix into the cecum becomes blocked. The blockage may be due to a build-up of thick mucus within the appendix or to stool that enters the appendix from the cecum. The mucus or stool hardens, becomes rock-like, and blocks the opening. This rock is called a “fecalith” (literally, a rock of stool). At other times, it might be that the lymphatic tissue in the appendix swells and blocks the opening. After the blockage occurs, bacteria which normally are found within the appendix begin to multiply and invade (infect) the wall of the appendix.
The body responds to the invasion by mounting an attack on the bacteria, an attack called inflammation. If the symptoms of appendicitis are not recognized and the inflammation progresses, the appendix can rupture, followed by spread of bacteria outside of the appendix. The cause of such a rupture is unclear, but it may relate to changes that occur in the lymphatic tissue that lines the wall of the appendix, for example, inflammation that causes swelling and buildup of pressure within the appendix that causes it to rupture.
After rupture, infection can spread throughout the abdomen; however, it usually is confined to a small area surrounding the appendix by the surrounding tissues, forming a peri-appendiceal abscess.
Sometimes, the body is successful in containing (“healing”) the appendicitis without surgical treatment if the infection and accompanying inflammation cause the appendix to rupture. The inflammation, pain, and symptoms also may disappear when antibiotics are used. This is particularly true in elderly patients. Patients then may come to the doctor long after the episode of appendicitis with a lump or a mass in the right lower abdomen that is due to the scarring that occurs during healing. This lump might raise the suspicion of cancer.
Acute appendicitis seems to be the end result of a primary obstruction of the appendix. Once this obstruction occurs, the appendix becomes filled with mucus and swells. This continued production of mucus leads to increased pressures within the lumen and the walls of the appendix. The increased pressure results in thrombosis and occlusion of the small vessels, and stasis of lymphatic flow. At this point spontaneous recovery rarely occurs.
As the occlusion of blood vessels progresses, the appendix becomes ischemic and then necrotic. As bacteria begin to leak out through the dying walls, pus forms within and around the appendix (suppuration). The end result is appendiceal rupture (a ‘burst appendix’) causing peritonitis, which may lead to sepsis and eventually death. These events are responsible for the slowly evolving abdominal pain and other commonly associated symptoms.
The causative agents include bezoars, foreign bodies, trauma, intestinal worms, lymphadenitis and, most commonly, calcified fecal deposits that are known as appendicoliths or fecoliths. The occurrence of obstructing fecaliths has attracted attention since their presence in people with appendicitis is higher in developed than in developing countries. In addition an appendiceal fecalith is commonly associated with complicated appendicitis. Fecal stasis and arrest may play a role, as demonstrated by people with acute appendicitis having fewer bowel movements per week compared with healthy controls.
The occurrence of a fecalith in the appendix was thought to be attributed to a right-sided fecal retention reservoir in the colon and a prolonged transit time. However, a prolonged transit time was not observed in subsequent studies. From epidemiological data, it has been stated that diverticular disease and adenomatous polyps were unknown and colon cancer exceedingly rare in communities exempt from appendicitis. And acute appendicitis has been shown to occur antecedent to cancer in the colon and rectum. Several studies offer evidence that a low fiber intake is involved in the pathogenesis of appendicitis. This low intake of dietary fiber is in accordance with the occurrence of a right-sided fecal reservoir and the fact that dietary fiber reduces transit time.
A blockage in the lining of the appendix that results in infection is the likely cause of appendicitis. The bacteria multiply rapidly, causing the appendix to become inflamed, swollen and filled with pus. If not treated promptly, the appendix can rupture.
For more information visit us our website: https://www.healthinfi.co
0 200
No Comments