Sjogren’s (SHOW-grins) syndrome is a disorder of your immune system identified by its two most common symptoms — dry eyes and a dry mouth.Although you can develop Sjogren’s syndrome at any age, most people are older than 40 at the time of diagnosis. The condition is much more common in women. Treatment focuses on relieving symptoms.
Women are nine times more likely than men to develop Sjögren’s syndrome, achronic, incurable disorder in whichimmune system cells attack and destroy the glands that produce moisture. Sjögren’s (pronounced “show-grins”) can occur at any age, but a woman is at higher risk for developing the condition after menopause.
The Sjögren’s Syndrome Foundation estimates that four million Americans suffer from this disorder; many go undiagnosed.
The syndrome, named after Swedish ophthalmologist Henrik Sjögren, is an autoimmune disorder—a disorder in which your immune system attacks your body’s healthy tissues. Ordinarily, the immune system produces antibodies and cells that target such destructive material as viruses and bacteria. In the case of Sjögren’s and other autoimmune diseases, the immune system produces autoreactive cells and autoantibodies, which turn against the part of the body they should protect.
The condition often accompanies other immune system disorders, such as rheumatoid arthritis and lupus. In Sjogren’s syndrome, the mucous membranes and moisture-secreting glands of your eyes and mouth are usually affected first — resulting in decreased tears and saliva.

Types of Sjogren Syndrome: Primary and Secondary
Sjögren’s syndrome may occur alone (referred to as primary Sjögren’s syndrome), or it may be associated with other autoimmune/rheumatic diseases, such as rheumatoid arthritis, lupus, polymyositis and scleroderma. When Sjögren’s occurs with another autoimmune disease it is called secondary Sjögren’s syndrome.
Symptoms of Sjogren Syndrome
Common Symptoms
Symptoms
-
Salivary glands
The two main symptoms of Sjogren’s syndrome are:
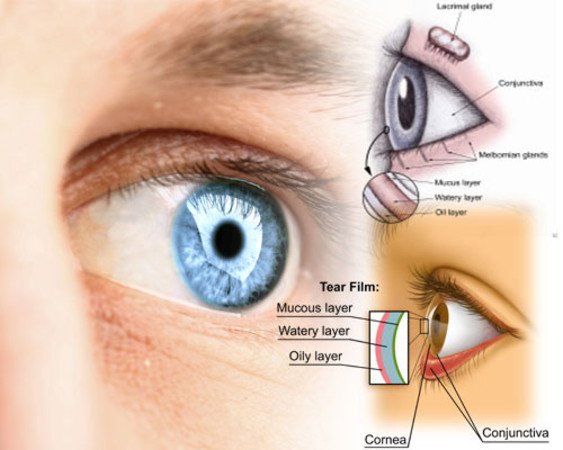
- Dry eyes. Your eyes might burn, itch or feel gritty — as if there’s sand in them.
- Dry mouth. Your mouth might feel like it’s full of cotton, making it difficult to swallow or speak.
Some people with Sjogren’s syndrome also have one or more of the following:
- Joint pain, swelling and stiffness
- Swollen salivary glands — particularly the set located behind your jaw and in front of your ears
- Skin rashes or dry skin
- Vaginal dryness
- Persistent dry cough
- Prolonged fatigue
Causes
Sjogren’s syndrome is an autoimmune disorder. Your immune system mistakenly attacks your body’s own cells and tissues.
Scientists aren’t certain why some people develop Sjogren’s syndrome. Certain genes put people at higher risk of the disorder, but it appears that a triggering mechanism — such as infection with a particular virus or strain of bacteria — is also necessary.
In Sjogren’s syndrome, your immune system first targets the glands that make tears and saliva. But it can also damage other parts of your body, such as:
- Joints
- Thyroid
- Kidneys
- Liver
- Lungs
- Skin
- Nerves
Risk factors
Sjogren’s syndrome typically occurs in people with one or more known risk factors, including:
- Age. Sjogren’s syndrome is usually diagnosed in people older than 40.
- Sex. Women are much more likely to have Sjogren’s syndrome.
- Rheumatic disease. It’s common for people who have Sjogren’s syndrome to also have a rheumatic disease — such as rheumatoid arthritis or lupus.
Complications
The most common complications of Sjogren’s syndrome involve your eyes and mouth.
- Dental cavities. Because saliva helps protect the teeth from the bacteria that cause cavities, you’re more prone to developing cavities if your mouth is dry.
- Yeast infections. People with Sjogren’s syndrome are much more likely to develop oral thrush, a yeast infection in the mouth.
- Vision problems. Dry eyes can lead to light sensitivity, blurred vision and corneal damage.
Less common complications might affect:
- Lungs, kidneys or liver. Inflammation can cause pneumonia, bronchitis or other problems in your lungs; lead to problems with kidney function; and cause hepatitis or cirrhosis in your liver.
- Lymph nodes. A small percentage of people with Sjogren’s syndrome develop cancer of the lymph nodes (lymphoma).
- Nerves. You might develop numbness, tingling and burning in your hands and feet (peripheral neuropathy).
The hallmark symptoms of Sjögren’s are dry eyes and dry mouth. The disorder may also cause skin, nose and vaginal dryness, and it can affect other organs of the body as well, including your skin, lungs, gastrointestinal tract, liver, pancreas, kidneys,thyroid, joints, muscles, blood, blood vessels, brain, spinal cord and peripheral nerves.
Inadequate tear production can result in eye irritation and a feeling of having grit or sand in your eyes. The lack of saliva generally causes dry mouth (xerostomia); this can lead to difficulties with speech and swallowing food, extensive tooth decay, tooth loss, oral sores and fungal infections in the mouth. If dry mouth is troublesome at night, it can cause sleep problems through a cycle of increased fluid intake and increased urination. The salivary glands may enlarge to produce visible swelling, particularly below the ears at the angle of the jaw; this swelling may be confused with mumps.
Another problem is that the quality of the saliva that is produced is not as good, predisposing you to problems related to oral bacteria. Saliva is the main protective factor for the upper gastrointestinal tract––the mouth, pharynx and esophagus. Salivary proteins help prevent tooth decay; repair wounds or ulcers in the soft mucous membrane tissues; kill bacteria, certain fungi and some viruses; and permit proper swallowing of food. Saliva also facilitates your ability to taste and to speak. All of these functions can be affected by Sjögren’s.
Impact of Sjogren Syndrome on Salivary Glands
Salivary glands are a prime target of Sjögren’s. They are composed of two parts, the acinar region or secretory end piece and the ductal region. Acinar cells are the site of fluid secretion, and they are responsible for making and secreting more than 85 percent of the proteins involved in producing saliva. Ductal cells cannot secrete fluid. In Sjögren’s, autoreactive lymphocytes (a type of white blood cell) infiltrate and destroy the glandular tissue.
Severe Symptoms
In severe cases, Sjögren’s can damage vital organs. Symptoms vary, as this is a disease of many manifestations. The symptoms may level out, worsen or go into remission (disappear for a while). Some people experience only the mild symptoms of dry eyes and mouth, while others experience cycles of good health followed by severe disease.
Many patients are able to treat problems symptomatically, but others must cope with blurred vision, constant eye discomfort, recurrent mouth infections, swollen parotid glands (the salivary glands near the ears), hoarseness, difficulty in swallowing and eating, bronchitis and other pulmonary disorders, debilitating fatigue and joint pain. Also, there is a slightly elevated risk of lymphoma in people with Sjögren’s.
Risks for Pregnant Women with Sjogren Syndrome
An autoantibody to the protein SS-A/Ro, found in women with Sjögren’s syndrome, can very rarely be associated with congenital heart block and neonatal lupus in newborn babies. If you have Sjögren’s syndrome and plan to become pregnant, see your health care professional about testing for this marker and deciding what to do if the marker is present.
Diagnosis
No single gene, microorganism or hormone is known to cause Sjögren’s syndrome. As a result, diagnosis is often difficult. Its symptoms can mimic those of other diseases, and no two people with Sjögren’s syndrome have exactly the same set of symptoms or medical history. Moreover, individual symptoms may be reported to different health care professionals—such as dry mouth to the dentist or dry eyes to an optometrist—so the condition often goes undiagnosed. In fact, the average time from the onset of Sjögren’s symptoms to diagnosis is over six years.
Once Sjögren’s is suspected, a detailed history and physical exam, blood tests for autoantibodies, tests to determine the degree of dry eye and mouth, and sometimes salivary gland biopsies, can point to the presence of Sjögren’s.
Tests can help rule out other conditions and help pinpoint a diagnosis of Sjogren’s syndrome.
Blood tests
Your doctor might order blood tests to check for:
- Levels of different types of blood cells
- Presence of antibodies common in Sjogren’s syndrome
- Evidence of inflammatory conditions
- Indications of problems with your liver and kidneys
Eye tests
Your doctor can measure the dryness of your eyes with a test called a Schirmer tear test. A small piece of filter paper is placed under your lower eyelid to measure your tear production.
A doctor specializing in the treatment of eye disorders (ophthalmologist) might also examine the surface of your eyes with a magnifying device called a slit lamp. He or she may place drops in your eye that make it easier to see damage to your cornea.
Imaging
Certain imaging tests can check the function of your salivary glands.
- Sialogram. This special X-ray can detect dye that’s injected into the salivary glands in front of your ears. This procedure shows how much saliva flows into your mouth.
- Salivary scintigraphy. This nuclear medicine test involves the injection into a vein of a radioactive isotope, which is tracked over an hour to see how quickly it arrives in all your salivary glands.
Biopsy
Your doctor might also do a lip biopsy to detect the presence of clusters of inflammatory cells, which can indicate Sjogren’s syndrome. For this test, a sliver of tissue is removed from salivary glands in your lip and examined under a microscope.
Symptoms can include:
- Dry mouth. If you have Sjögren’s syndrome, you produce far less saliva than normal. This makes chewing, swallowing and speaking difficult, and it may diminish your sense of taste as well as produce halitosis, or bad breath.
- Dry eyes. Your eyes may feel dry and gritty—they may also burn and turn red and be extre me ly sensitive to sunlight. A thick substance may accumulate in the inner corner of your eyes while you sleep. If not properly treated, Sjögren’s syndro me can so metimes lead to ulcers of the cornea. On rare occasions, this can cause loss of vision.
- Swollen salivary glands. Two sets of major salivary glands produce saliva. They are under your tongue and in the cheeks in front of your ears. They may feel swollen and tender.
- Dental cavities. Saliva fights bacteria and defends against cavities. If you have Sjögren’s syndrome, your saliva will be decreased, and your teeth may develop cavities more easily.
- Dry nose, throat and lungs. Your throat feels dry and tickly, and you may have a dry cough, hoarseness, a decreased sense of smell and nosebleeds. Sjögren’s can also lead to pneumonia, bronchitis and ear problems.
- Vaginal dryness. Because Sjögren’s can affect the me chanisms for secreting vaginal fluids, you may find sexual penetration difficult.
- Fatigue. Sjögren’s may cause you to tire more easily or feel an underlying fatigue. Fatigue is also frequently a symptom of other autoimmune disorders, such as rheumatoid arthritis or lupus.
- Joint pain. If the immune system attack spreads to the joints, move me nt of fingers or other joints can become difficult or painful. Joint involvement may indicate you have another autoimmune disorder, such as rheumatoid arthritis or lupus.
- Other problems. Sjögren’s syndrome can affect other parts of the body, such as blood vessels, the nervous system, muscles, skin and other organs. This can lead to muscle weakness, confusion and me mory problems, dry skin and feelings of numbness and tingling. Sjögren’s syndrome can also affect the liver and spleen. People with Sjögren’s also have a slightly increased risk of developing lymphoma (cancer of the lymphocytes). Although this is unusual, it is another reason why medical exams and continued follow-up are critical.
With such a broad array of symptoms, in varying severity from patient to patient, diagnosis can be difficult. You and your health care professional may go through several steps before confirming the diagnosis of Sjögren’s syndrome.
- Medical history and physical examination. Your health care professional will probably ask you to describe your symptoms. He or she will then look for other signs of Sjögren’s, such as red, itchy eyes; swollen salivary glands; a dry, cracked tongue; and enlarged salivary glands in your neck. You’ll also want to discuss what me dications you are taking—both prescription and over-the-counter, because many medications can cause dryness of the mouth and eyes.
- Blood tests. Antinuclear antibodies ( ANA ), a group of antibodies that react against normal components of a cell nucleus , may be found in patients with Sjögren’s syndrome, as well as the antibodies SS-A (or Ro) and SS-B (or La). However, not everyone with Sjögren’s has these markers, and not everyone with these markers has Sjögren’s syndrome.
- Schirmer test. This helps determine how dry your eyes are. It involves placing a small piece of filter paper under your lower eyelid to measure tear production.
- Rose Bengal and Lissamine Green and sodium fluorescein. These dyes are used to detect dry spots on the surface of the eye.
- Salivary gland biopsy. In this test, the health care professional removes a few minor salivary glands, usually from inside your lower lip. The tissue is examined under a microscope. The appearance of the tissue helps determine if you have Sjögren’s syndrome.
- Salivary function tests. To measure the amount of saliva you produce over a certain time, your health care professional may order tests such as a salivary scintigraphy, which involves injection of a radioactive isotope, or a sialography, an x-ray of the salivary-duct system that shows how much saliva flows into your mouth. He or she may also order a spit test, during which you spit into a test tube every minute for 15 minutes, to measure your saliva production.
- Urine tests. These may be done to test your kidney function.
- Chest x-ray. This can help detect inflammation in the lungs.
Treatment
Treatment for Sjogren’s syndrome depends on the parts of the body affected. Many people manage the dry eye and dry mouth of Sjogren’s syndrome by using over-the-counter eyedrops and sipping water more frequently. But some people need prescription medications, or even surgical procedures.
Medications
Depending on your symptoms, your doctor might suggest medications that:
- Decrease eye inflammation. Prescription eyedrops such as cyclosporine (Restasis) or lifitegrast (Xiidra) may be recommended by your eye doctor if you have moderate to severe dry eyes.
- Increase production of saliva. Drugs such as pilocarpine (Salagen) and cevimeline (Evoxac) can increase the production of saliva, and sometimes tears. Side effects can include sweating, abdominal pain, flushing and increased urination.
- Address specific complications. If you develop arthritis symptoms, you might benefit from nonsteroidal anti-inflammatory drugs (NSAIDs) or other arthritis medications. Yeast infections in the mouth should be treated with antifungal medications.
- Treat systemwide symptoms. Hydroxychloroquine (Plaquenil), a drug designed to treat malaria, is often helpful in treating Sjogren’s syndrome. Drugs that suppress the immune system, such as methotrexate (Trexall), also might be prescribed.
There is no cure for Sjögren’s syndrome, and no treatment has yet been found to restore physiological glandular secretions. This means that treatment primarily addresses the symptoms and is designed to relieve your discomfort and lessen the effects of dryness. Put another way, you can generally learn to manage your condition, but the root problems will remain. You may be referred to a rheumatologist for treatment.
Sjögren’s syndrome can affect various parts of your body, so regular checkups can help detect and prevent future problems. And if you have secondary Sjögren’s syndrome—that is, if the disorder is associated with another autoimmune condition—be sure to follow treat me nts for that condition.
Since Sjögren’s syndrome affects everyone differently, your treatment plan will be based on your specific needs. But in general, moisture-replacement therapies may ease the symptoms of dryness. In some cases, your health care professional may recommend a simple procedure that blocks tear drainage from your eyes.
Dry eyes respond to the use of artificial tears or to pharmacological stimulation of tear production. Dry mouth can be relieved by drinking water, chewing sugar-free gum or using artificial saliva or saliva stimulants (such as pilocarpine and cevimeline). Wearing protective eyewear, such as goggles, or using a humidifier to keep moisture in the air can be helpful.
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen, may be used to treat musculoskeletal symptoms. If you have severe complications, your health care professional may prescribe corticosteroids and/or immunosuppressive drugs.
Here’s an overview of some of the most commonly used medications:
- NSAIDs can suppress inflammation and reduce pain. Sjögren’s patients are generally prescribed NSAIDs for joint pain, muscle ache, fever and fatigue. However, NSAIDs provide no improvement in the salivary or tear flow.
- Corticosteroids may be used if you have internal organ involvement, which is rare. If you have secondary Sjögren’s syndrome, you may already be on corticosteroids––especially if the primary condition is lupus or rheumatoid arthritis. The side effects can be significant, so you and your health care professional need to monitor both the effectiveness and possible side effects of the medication.
- Hydroxychloroquine (Plaquenil), an antimalarial drug, is sometime used to relieve swelling, stiffness and pain. It may also have a limited effect on the glandular symptoms, the hallmark of the disease.
- Immunomodulating agents are occasionally used in autoimmune diseases like Sjögren’s. These medications act very slowly, so they don’t bring about immediate relief. As with corticosteroids, these immunomodulating agents are generally used when there is internal organ involvement. These agents can include:
- Methotrexate (Trexall) is a folic-acid inhibitor generally used to treat rheumatoid arthritis and may be prescribed in rare cases for Sjögren’s patients with internal organ involvement.
- Cyclophosphamide (Cytoxan) is considerably more potent than methotrexate and is reserved for the most serious organ involvement. Other drugs used for severe organ involvement include mycophenolate (CellCept) and azathioprine (Azasan, Imuran).
- Antifungal drugs, such as nystatin (Bio-Statin) may be used to treat oral candidiasis (a common fungal infection).
- Pilocarpine (Salagen) and cevimeline (Evoxac) tablets may be used to increase salivary flow. Evoxac, however, should not be used for those with a number of other conditions, including asthma and acute angle glaucoma. Higher doses of both of these medications may have significant side effects including flushing, sweating, nausea, vomiting and diarrhea, among others.
- Saliva substitutes such as Oasis Mouth Moisturizing Spray, Mouth Kote spray and Biotene mouth spray and gel, can be used to replace oral secretions.
- Artificial tears or eyedrops can help relieve the discomfort of dry eyes. You probably want to use preservative-free products, especially if you apply the drops frequently. These products include Tears Naturale Free and Bion Tears. (Note: Some over-the-counter eyedrops contain vasoconstrictors and can cause further drying.)
- Cyclosporine A (Restasis) eyedrops decrease inflammation and are also used to increase tear production. Unlike artificial tears, these are available only by prescription.
- Hydroxypropyl cellulose (Lacrisert), a small dissolvable cellulose pellet that fit into your lower eyelid, may also be helpful in the treatment of dry eyes. Lacrisert is also only available by prescription.
Prevention
Sadly, there’s no known way to prevent the onset of Sjögren’s syndrome. However, the symptoms are often treatable, and you can develop strategies for keeping some symptoms at bay.
Early diagnosis and intervention may slow the progress of Sjögren’s syndrome and prevent complications. All too often, the condition goes undiagnosed and symptoms continue to worsen. Since Sjögren’s syndrome can affect many parts of the body, regular checkups can help detect and prevent problems. You and your health care professional should meet frequently to discuss your treatment strategy to keep the condition from worsening.
A healthy diet is part of taking care of yourself under any circumstances, and it’s doubly important if you have Sjögren’s. You should probably avoid alcoholic and caffeinated beverages because they may be dehydrating. Spicy and acidic food can irritate your mouth, and sugary food can promote tooth decay.
Of course, get plenty of rest and avoid tobacco and (when possible) stress. Mild exercise, such as walking or swimming, can help keep joints and muscles flexible. Exercise may also protect against further joint damage. Warm compresses or heating pads can help ease joint or gland pain.
Keeping your mouth moist is important. Artificial moisture can help. Methylcellulose swabs or spray may help alleviate mouth dryness and lower your risk of ulcers. Sipping sugar-free fluids throughout the day may help, too, as well as sugar-free gum or candies, which stimulate saliva production. Use artificial tears or eyedrops to relieve the discomfort of dry eyes. Medications such as Salagen and Evoxac may improve saliva production, and eyedrops containing cyclosporine A (Restasis) may improve tear production.
Practicing good oral hygiene is essential. Frequent dental checkups, fluoride and mouth rinses, regular brushing with antibacterial toothpastes and flossing are more important for Sjögren’s patients, since you are at a higher risk for tooth decay.
Here are other coping strategies that can help moderate your symptoms.
- Don’t smoke; avoid tobacco smoke and other air irritants.
- Use self-adhesive stamps and envelopes.
- Don’t direct hair dryers toward your eyes.
- Wear glasses on windy days and goggles when swimming.
- Coat your lips with petroleum-based lubricants to prevent drying. (Many lipsticks can also provide this protection.)
- Keep your home humidity between 30 percent and 50 percent. You may want to use a humidifier year-round. Some experts advise using a cool-mist, ultrasonic humidifier; be sure to clean it daily.
- Avoid rubbing your eyes.
- If you have nasal and airway dryness, consider using a soft cervical collar while you sleep to help prevent your mouth from opening, thus preventing the dryness that mouth breathing causes.
- Avoid abrasive detergents, soaps and, in some cases, dryer sheets.
- Consider soft contact lenses rather than the traditional hard ones. Many patients with Sjögren’s are unable to wear contact lenses.
- Avoid prolonged hot showers or baths.
- Talk to your health care professional about discontinuing your use of decongestants and antihistamines because they dry your mouth and nasal areas.
- Use sunscreen.
- Apply lotions or other lubricants to still-damp skin right after you bathe or shower.
- Frequent small sips of water—or sucking on ice chips—can help keep your lips and gastrointestinal tract hydrated.
- Avoid drafts from air conditioners, heaters and radiators, when possible.
- If you have vaginal dryness, use lubricants made specifically for that purpose.
Finally, experts stress the importance of mental and emotional health. Joining a self-help or support group can help you cope emotionally, as well as teach you new strategies for managing your disease.
Facts to Know
- Women are nine times more likely than men to develop Sjögren’s (pronounced “show-grins”) syndrome, a chronic, incurable disorder in which immune system cells attack and destroy the glands that produce tears and saliva. Sjögren’s can occur at any age, but women are at higher risk after menopause.
- The hallmark symptoms of Sjögren’s are dry eyes and dry mouth. The disorder may also cause skin, nose and vaginal dryness, and, in rare cases, affect other organs of the body as well, including your kidneys, blood vessels, lungs, liver, pancreas and brain.
- The Sjögren’s Syndrome Foundation estimates that four million Americans suffer from this disorder; many go undiagnosed.
- The syndrome, named after Swedish ophthalmologist Henrik Sjögren, is an autoimmune disorder, which means that your immune system attacks your body’s healthy tissues. Ordinarily, the immune system produces antibodies that target such destructive material as viruses and bacteria. In the case of Sjögren’s and other autoimmune diseases, autoantibodies—antibodies turned against the self—are produced.
- Sjögren’s syndrome may occur alone (primary Sjögren’s syndrome), or it may be a symptom of other autoimmune/rheumatic diseases, such as rheumatoid arthritis, lupus, polymyositis and some forms of scleroderma (secondary Sjögren’s syndrome).
- A blood marker often found in women with Sjögren’s syndrome can, very rarely, be associated with heart problems or neonatal lupus in newborn babies. If you have Sjögren’s syndrome and plan to become pregnant, see your health care professional about testing for this marker and deciding what to do if the marker is present.
- There is no cure for Sjögren’s syndrome, and no treatment has yet been found to restore total glandular secretions. This means that treatment addresses the symptoms only and is designed to relieve your discomfort and lessen the effects of dryness. Put another way, you can generally learn to manage your condition, but the root problems will remain.
- Much about Sjögren’s is still unknown. Certain genes seem to put people at a higher risk for the disorder, but scientists think some sort of a trigger—such as a virus or bacteria—is also necessary to bring it on. Unfortunately, there’s no way to prevent the onset of Sjögren’s syndrome. However, the symptoms are often treatable, and you can develop strategies for keeping some symptoms at bay.
- A healthy diet is part of taking care of yourself under any circumstances, and it’s doubly important if you have Sjögren’s. You should probably avoid alcoholic and caffeinated beverages because they are dehydrating. Spicy and acidic food can also irritate your mouth, and sugary food can promote tooth decay.
- Since Sjögren’s syndrome affects everyone differently, your treatment plan will be based on your specific needs. In general, moisture-replacement therapies may ease the symptoms of dryness. In some cases, your health care professional may recommend a simple operation that blocks tear drainage from your eye.
Key Q&A
- Who gets Sjögren’s syndrome? Am I at risk?Women are nine times more likely to develop Sjögren’s syndrome than men, and the disorder occurs sometimes in connection with another autoimmune disease, such as rheumatoid arthritis, lupus or scleroderma. Women are at higher risk for developing Sjögren’s after menopause. And the disorder sometimes runs in families. Other than those, there are no clear risk factors for predicting who will get Sjögren’s.
- How can I prevent the disease?Researchers have not found any special dietary guidelines or lifestyle modifications that can stave off the onset of Sjögren’s. The best that can be done is to diagnose the disease as early as possible and start aggressive treatment to try to prevent worsening of symptoms.
- Why is Sjögren’s called an autoimmune disease?Ordinarily, the immune system produces antibodies that target such destructive material as viruses and bacteria. In the case of Sjögren’s and other autoimmune diseases, autoantibodies—antibodies that turn against the part of the body they should protect—are produced. With Sjögren’s, immune-system cells attack and destroy the glands that produce tears and saliva.
- What are the symptoms of Sjögren’s?The hallmark symptoms of Sjögren’s are dry eyes and dry mouth. The disorder may also include skin, nose and vaginal dryness, as well as swollen salivary glands, joint pain and fatigue.
- I have dry mouth and dry eyes. Do I really need to see a health care professional, or can I just use artificial tears and sip water?Early diagnosis and a systematic treatment plan are essential for slowing the disease’s progress. Sjögren’s syndrome can affect other parts of the body, such as blood vessels, the nervous system, muscles, skin and other organs. This can lead to muscle weakness, confusion and memory problems, dry skin and feelings of numbness and tingling. When Sjögren’s syndrome affects other organs, there is a greater chance for developing cancer of the lymph tissue. Although this is unusual, it is another reason why medical exams and continued follow-up are critical.
- How is Sjögren’s syndrome diagnosed?Once Sjögren’s is suspected, blood tests for autoantibodies, tests to determine the degree of dry eye and mouth and sometimes salivary gland biopsies can point to the presence of Sjögren’s.
- Is it safe to get pregnant if I have Sjögren’s?A blood marker often found in women with Sjögren’s syndrome can, very rarely, be associated with heart problems or neonatal lupus in newborn babies. If you have Sjögren’s syndrome and plan to become pregnant, see your health care professional about testing for this marker and deciding what to do if the marker is present.
- What treatments are available for Sjögren’s?Artificial tears, which are sold under many brand names, combat dry eyes, and saliva substitutes (such as Oasis Mouth Moisturizing Spray, Mouth Kote spray and Biotene mouth spray and gel) combat dry mouth. If you need to use artificial tears more than four times a day, it is best to use preservative-free drops because preservatives can irritate dry eyes. Talk to your health care professional before using any of these products.
- Cyclosporine A (Restasis) eyedrops decrease inflammation and are also used to increase tear production. Unlike artificial tears, these are available only by prescription. Over-the-counter lubricating products are also available to address vaginal, skin and nasal dryness. Pilocarpine (Salagen) or cevimeline (Evoxac) tablets may be prescribed to increase salivary flow. If symptoms include joint pain, muscle ache, fever and fatigue, nonsteroidal anti-inflammatory drugs such as aspirin or ibuprofen may be prescribed or recommended. In a case of internal organ involvement, your health care professional may recommend more aggressive treatments, such as corticosteroids and/or immunomodulating agents.
For more information visit us our website: https://www.healthinfi.com
0 200

Visitor Rating: 1 Stars