
Bancroftian Filariasis
Wuchereria bancrofti is a human parasitic roundworm that is the major cause of lymphatic filariasis. It is one of the three parasitic worms, together with Brugia malayi and B. timori, that infect the lymphatic system to cause lymphatic filariasis. These filarial worms are spread by a variety of mosquito vector species. W. bancrofti is the most prevalent of the three and affects over 120 million people, primarily in Central Africa and the Nile delta, South and Central America,
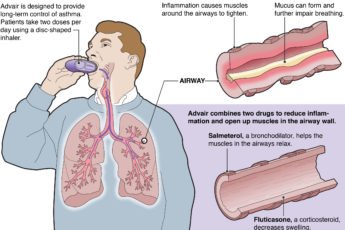
the tropical regions of Asia including southern China, and the Pacific islands. If left untreated, the infection can develop into a chronic disease called elephantiasis. In rare conditions it also causes tropical eosinophilia, an asthmatic disease.
There is no commercially available vaccine, however high rates of cure have been achieved with various anti-filarial regimens and lymphatic filariasis is the target of the WHO Global Program to Eliminate Lymphatic Filariasis with the aim to eradicate the disease as a public health problem by 2020.
In the human body the female nematode gives birth to elongated embryos, the microfilariae, which migrate through the peripheral blood and skin, from which they are taken by bloodsucking insects. Within the insect carrier, the microfilariae grow into motile, infective larvae that, at the insect’s next blood meal, are introduced into the human host, where they reach maturity in about a year.
The term filariasis is commonly used to designate bancroftian filariasis, caused by Wuchereria bancrofti, organisms that are widely distributed in tropical and subtropical regions of the world and are transmitted to man by mosquitoes, usually Culex fatigans. The nematode lives principally in the lymph nodes and lymph vessels, notably those draining the legs and genital area, where the adult worms induce allergic reactions in the sensitized tissues.
The initial inflammatory stage is characterized by granulomatous lesions, swelling, and impaired circulation; this stage is followed by enlargement of the lymph nodes and dilation of the lymph channels, which, over the years, harden and become infiltrated and clogged with fibrous tissue elements, resulting in some of the untreated cases in the condition known as elephantiasis, which is typically associated with the gross expansion of the tissues of the legs and scrotum. The most effective therapeutic drugs are diethylcarbamazine and sodium caparsolate, which kill the adult worms and microfilariae.
The form of filariasis known as filariasis malayi closely resembles bancroftian filariasis in its symptoms and pathological changes; it is caused by Brugia malayi, found chiefly in the Far East. Onchocerciasis (river blindness) is caused by Onchocerca volvulus, which is transmitted to man by flies of the genus Simulium, which breed along fast-moving streams; the condition is widespread in southern Mexico and Guatemala and is common in Central Africa. Characteristic lesions are nodules beneath the skin, usually in the head region; the infection may also invade the eyes, causing blindness in about 5 percent of the infected individuals.
Treatment consists of the surgical excision of the nodules and the administration of chemotherapeutics. Loiasis, prevalent in West and Central Africa, especially along the Congo River, is caused by Loa loa and transmitted by flies of the genus Chrysops. It is characterized by transient areas of allergic inflammation in the tissues beneath the skin, called calabar swellings; adult worms may sometimes be visible beneath the conjunctiva (the delicate membrane lining the eyelids and covering the exposed surface of the eyeball).
Loiasis produces irritation but seldom permanent damage. Treatment includes surgical removal of the worms from the conjunctiva and drug therapy. Other forms of filariasis are caused by Acanthocheilonema perstans and Mansonella ozzardi and are not in most cases associated with specific symptoms. The prevention of filariasis relies heavily on insecticides and insect repellents.
Lymphatic filariasis is infection with any of 3 species of Filarioidea. Acute symptoms include fever, lymphadenitis, lymphangitis, funiculitis, and epididymitis. Chronic symptoms include abscesses, hyperkeratosis, polyarthritis, hydroceles, lymphedema, and elephantiasis. Tropical pulmonary eosinophilia with bronchospasm, fever, and pulmonary infiltrates is another manifestation of infection. Diagnosis is by detection of microfilariae in blood, ultrasound visualization of adult worms, or serologic testing. Treatment is with diethylcarbamazine; antibiotics are used for complicating bacterial cellulitis.
In order to use a combination of ivermectin and albendazole for the elimination of lymphatic filariasis, it is important to assess the potential risk of increased adverse events in individuals infected with both lymphatic filariasis and onchocerciasis. We compared the safety and efficacy of albendazole (400 mg) in combination with ivermectin (150 micrograms/kg), for the treatment of co-infections of Wuchereria bancrofti and Onchocerca volvulus with single infection of W. bancrofti.
Filariasis is a disease group caused by filariae that affects humans and animals (ie, nematode parasites of the family Filariidae). [1] Of the hundreds of described filarial parasites, only 8 species cause natural infections in humans. The World Health Organization (WHO) has identified lymphatic filariasis as a major cause of disability worldwide, with an estimated 40 million individuals affected by the disfiguring features of the disease. [2]
In lymphatic filariasis, repeated episodes of inflammation and lymphedema lead to lymphatic damage, chronic swelling, and elephantiasis of the legs (see the image below), arms, scrotum, vulva, and breasts.
Presently, there is inadequate information on the geographical distribution and burden of disease of lymphatic filariasis in Africa on which to establish elimination programmes. A recent review of published and reported filariasis surveys showed that only few areas, notably the East African coast and Madagascar, were well surveyed with respect to infection prevalence. Information on the distribution of filariasis is a pre-requisite for advocacy and planning for filariasis elimination programmes. This has become increasingly evident during several meetings during 1999, culminating in the joint OCP and APOC board meeting to discuss possible synergism between the programmes for elimination of lymphatic filariasis and the onchocerciasis control programmes. The urgent need to better understand the geographical distribution of lymphatic filariasis in Africa is recognised by all concerned and mapping the distribution of the disease is a top priority as prerequisite for action against lymphatic filariasis.
This document provides operational guidelines for rapid mapping of lymphatic filariasis in Africa. A standardized methodology for rapid mapping of lymphatic filariasis has been developed, based on previous work on rapid mapping (section 3) and extensive consultation with partners on the optimal approach.
The last stage in the consultative process was an inter-country workshop with participants from the Ministries of Health of 7 African countries. The standard methodology, as agreed upon during the workshop, is described in section 4, and specific comments of the participants, based on their first experience with the method, are given in section 5. The final two sections of the document provide a proposal for the phased implementation of filariasis mapping in Africa.
Lymphatic filariasis (LF) is one of the most debilitating neglected tropical diseases (NTDs). It still presents as an important public health problem in many countries in the tropics. In Cameroon, where many NTDs are endemic, only scant data describing the situation regarding LF epidemiology was available. The aim of this study was to describe the current situation regarding LF infection in Cameroon, and to map this infection and accurately delineate areas where mass drug administration (MDA) was required
Symptoms
Infection can result in microfilaremia without overt clinical manifestations. Symptoms and signs are caused primarily by adult worms. Microfilaremia gradually disappears after people leave the endemic area.
Acute inflammatory filariasis consists of 4- to 7-day episodes (often recurrent) of fever and inflammation of lymph nodes with lymphangitis (termed acute adenolymphangitis [ADL]) or acute epididymitis and spermatic cord inflammation. Localized involvement of a limb may cause an abscess that drains externally and leaves a scar. ADL is often associated with secondary bacterial infections. ADL episodes usually precede onset of chronic disease by ≥ 2 decades. Acute filariasis is more severe in previously unexposed immigrants to endemic areas than in native residents.
Chronic filarial disease develops insidiously after many years. In most patients, asymptomatic lymphatic dilation occurs, but chronic inflammatory responses to adult worms and secondary bacterial infections may result in chronic lymphedema of the affected body area. Increased local susceptibility to bacterial and fungal infections further contributes to its development. Chronic pitting lymphedema of a lower extremity can progress to elephantiasis (chronic lymphatic obstruction). W. bancrofti can cause hydrocele and scrotal elephantiasis. Other forms of chronic filarial disease are caused by disruption of lymphatic vessels or aberrant drainage of lymph fluid, leading to chyluria and chyloceles.
Extralymphatic signs include chronic microscopic hematuria and proteinuria and mild polyarthritis, all presumed to result from immune complex deposition.
Tropical pulmonary eosinophilia (TPE) is an uncommon manifestation with recurrent bronchospasm, transitory lung infiltrates, low-grade fever, and marked eosinophilia. It is most likely due to hypersensitivity reactions to microfilariae. Chronic TPE can lead to pulmonary fibrosis.
Diagnosis
- Microscopic examination of blood samples
- Antigen test for W. bancrofti
- Antibody tests
Microscopic detection of microfilariae in blood establishes the diagnosis of lymphatic filariasis. Filtered or centrifuged concentrates of blood are more sensitive than thick blood films. Blood samples must be obtained when microfilaremia peaks—at night in most endemic areas, but during the day in many Pacific islands. Viable adult worms can be visualized in dilated lymphatics by ultrasonography; their movement has been called the filarial dance.
Several blood tests are available:
- Antigen detection: A rapid-format immunochromatographic test for W. bancrofti antigens
- Molecular diagnosis: Polymerase chain reaction assays for W. bancrofti and B. malayi
- Antibody detection: Alternatively, enzyme immunoassay tests for antifilarial IgG1 and IgG4
Patients with active filarial infection typically have elevated levels of antifilarial IgG4 in the blood. However, there is substantial antigenic cross-reactivity between filariae and other helminths, and a positive serologic test does not distinguish between past and current infection.
A blood smear is a simple and fairly accurate diagnostic tool, provided the blood sample is taken during the period in the day when the juveniles are in the peripheral circulation.[11] Technicians analyzing the blood smear must be able to distinguish between W. bancrofti and other parasites potentially present.
A polymerase chain reaction test can also be performed to detect a minute fraction, as little as 1 pg, of filarial DNA.[12]
Some infected people do not have microfilariae in their blood. As a result, tests aimed to detect antigens from adult worms can be used.
Ultrasonography can also be used to detect the movements and noises caused by the movement of adult worms.[13]
Dead, calcified worms can be detected by X-ray examinations.
Treatment
Diethylcarbamazine
Diethylcarbamazine (DEC) kills microfilariae and a variable proportion of adult worms. In the US, DEC is available only from the CDC after laboratory confirmation of filariasis
Treatment of acute lymphatic filariasis
DEC 2 mg/kg po tid for 12 days has traditionally been used; 6 mg/kg po once is an alternative. Generally, the 1-day regimen seems to be as effective as the 12-day regimen.
Adverse effects with DEC are usually limited and depend on the number of microfilariae in the blood. The most common are dizziness, nausea, fever, headache, and pain in muscles or joints, which are thought to be related to release of filarial antigens.
Before treatment with DEC, patients should be assessed for coinfection with Loa loa (loiasis) and Onchocerca volvulus (onchocerciasis) because DEC can cause serious reactions in patients with those infections. A single dose of albendazole 400 mg po plus ivermectin (200 mcg/kg po) in areas where onchocerciasis is co-endemic or DEC (6 mg/kg) in areas without onchocerciasis and loiasis rapidly reduces microfilaremia levels, but ivermectin does not kill adult worms.
A number of drug combinations and regimens have been used in mass treatment programs.
Also, doxycycline has been given long-term (eg, 100 mg po bid for 4 to 8 wk). Doxycycline kills Wolbachia endosymbiont bacteria within filaria, leading to death of adult filarial worms. It can be given with DEC or used alone.
Acute attacks of ADL usually resolve spontaneously, although antibiotics may be required to control secondary bacterial infections.
Treatment of chronic lymphedema
Chronic lymphedema requires meticulous skin care, including use of systemic antibiotics to treat secondary bacterial infections; these antibiotics may slow or prevent progression to elephantiasis. Whether DEC therapy prevents or lessens chronic lymphedema remains controversial. Conservative measures such as elastic bandaging of the affected limb reduce swelling.
Surgical decompression using nodal-venous shunts to improve lymphatic drainage offers some long-term benefit in extreme cases of elephantiasis. Massive hydroceles can also be managed surgically.
The severe symptoms caused by the parasite can be avoided by cleansing the skin, surgery, or the use of anthelmintic drugs, such as diethylcarbamazine (DEC), ivermectin, or albendazole. The drug of choice is DEC, which can eliminate the microfilariae from the blood and also kill the adult worms with a dosage of 6 mg/kg semiannually or annually. A polytherapy treatment that includes ivermectin with DEC or albendazole is more effective than each drug alone. Protection is similar to that of other mosquito-spread illnesses; one can use barriers both physical (a mosquito net), chemical (insect repellent), or mass chemotherapy as a method to control the spread of the disease.
Mass chemotherapy should cover the entire endemic area at the same time. This will significantly decrease the overall microfilarial titer in blood in mass, hence decreasing the transmission through mosquitoes during their subsequent bites.
Antibiotic active against the Wolbachia symbionts of the worm have been experimented with as treatment. Wolbachia-free worms immediately become sterile, and later die prematurely.
Methods
The study was conducted in Tanga region in Northeastern Tanzania along the Indian Coast (05°04′S, 39°06′E). The region is characterised mainly by two rain seasons annually: the long rains from March to June and the less intensive short rains from November to December. The majority of the inhabitants practice subsistence farming, fishing, and livestock keeping. The climate in Tanga region is warm and wet. In most cases, there is no big variation of temperature at the coast due to the influence of the Indian Ocean. Also, the region is characterised by high humidity, which often goes up to 100% maximum and ranges from 65 to 70% minimum.
There are health facilities in most villages in the regions, and the majority of the population have access to a health facility within a distance of 6 km. Most of the houses are made of mud walls with their roofs thatched with dried coconut leaves. This makes it easier for the vector to penetrate. Bancroftian filariasis control started in 2004 using MDA campaigns and advocacy with ivermectin and albendazole in all districts. The estimated population size of the area was 2,045,205 inhabitants according to 2012 national census survey.
0 200
No Comments